Beruflich Dokumente
Kultur Dokumente
Thomee - Patellofemoral Pain Syndrome
Hochgeladen von
KtomislavCopyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Thomee - Patellofemoral Pain Syndrome
Hochgeladen von
KtomislavCopyright:
Verfügbare Formate
REVIEW ARTICLE
Sports Med 1999 Oct; 28 (4): 245-262
0112-1642/99/0010-0245/$09.00/0
Adis International Limited. All rights reserved.
Patellofemoral Pain Syndrome
A Review of Current Issues
Roland Thome,1 Jesper Augustsson1 and Jon Karlsson2
1 Muscle Laboratory, Department of Rehabilitation Medicine, Sahlgrenska University Hospital,
Gteborg, Sweden
2 Department of Orthopaedics, Sahlgrenska University Hospital, Gteborg, Sweden
Contents
Abstract
. . . . . . . . . . . . . . . . . . . . . . . .
1. Definition of Patellofemoral Pain Syndrome (PFPS)
2. The Patellofemoral Joint . . . . . . . . . . . . . . . .
2.1 Anatomy and Biomechanics . . . . . . . . . .
2.2 Cartilage Properties . . . . . . . . . . . . . . .
3. Incidence of PFPS . . . . . . . . . . . . . . . . . . .
4. Aetiology of PFPS . . . . . . . . . . . . . . . . . . . .
4.1 Malalignment . . . . . . . . . . . . . . . . . . .
4.2 Muscular Imbalance . . . . . . . . . . . . . . .
4.3 Overactivity . . . . . . . . . . . . . . . . . . . .
5. Symptoms . . . . . . . . . . . . . . . . . . . . . . . .
5.1 Pain . . . . . . . . . . . . . . . . . . . . . . . .
6. Treatment . . . . . . . . . . . . . . . . . . . . . . . .
6.1 Patellar Taping . . . . . . . . . . . . . . . . . .
6.2 Surgical Treatment . . . . . . . . . . . . . . . .
7. Conclusion . . . . . . . . . . . . . . . . . . . . . . .
Abstract
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
245
246
247
247
247
248
248
248
250
251
252
252
254
256
257
258
There is no clear consensus in the literature concerning the terminology, aetiology and treatment for pain in the anterior part of the knee. The term anterior
knee pain is suggested to encompass all pain-related problems. By excluding
anterior knee pain due to intra-articular pathology, peripatellar tendinitis or bursitis,
plica syndromes, Sinding Larsens disease, Osgood Schlatters disease, neuromas
and other rarely occurring pathologies, it is suggested that remaining patients
with a clinical presentation of anterior knee pain could be diagnosed with patellofemoral pain syndrome (PFPS). Three major contributing factors of PFPS are
discussed: (i) malalignment of the lower extremity and/or the patella; (ii) muscular imbalance of the lower extremity; and (iii) overactivity.
The significance of lower extremity alignment factors and pathological limits
needs further investigation. It is possible that the definitions used for malalignment should be re-evaluated, as the scientific support is very weak for determining
when alignment is normal and when there is malalignment. Consequently, pathological limits must be clarified, along with evaluation of risk factors for acquiring
PFPS.
Muscle tightness and muscular imbalance of the lower extremity muscles with
246
Thome et al.
decreased strength due to hypotrophy or inhibition have been suggested, but
remain unclear as potential causes of PFPS. Decreased knee extensor strength is
a common finding in patients with PFPS. Various patterns of weaknesses have
been reported, with selective weakness in eccentric muscle strength, within the
quadriceps muscle and in terminal knee extension. The significance of muscle
function in a closed versus open kinetic chain has been discussed, but is far from
well investigated. It is clear that further studies are necessary in order to establish
the significance of various strength deficits and muscular imbalances, and to
clarify whether a specific disturbance in muscular activation is a cause or an effect
(or both) of PFPS.
The most common symptoms in patients with PFPS are pain during and after
physical activity, during bodyweight loading of the lower extremities in walking
up/down stairs and squatting, and in sitting with the knees flexed. However, the
source of patellofemoral pain in patients with PFPS cannot be sufficiently explained. There are several types of clinical manifestation of pain, and therefore a
differentiated documentation of the patients pain symptoms is necessary. The
connection between strength, pain and inhibition, as well as between personality
and pain, needs further investigation.
Many different treatment protocols are described in the literature and recent
studies advocate a comprehensive treatment approach allowing for an individual
and specifically designed treatment. Surgical treatment is rarely indicated.
It is strongly suggested that, when presenting studies on PFPS, a detailed
description should be provided of the diagnosis, inclusion and exclusion criteria
of the patients should be specified along with a detailed methodology, and the
conclusions drawn should be compared with those of other studies in the published
literature. As this is not the case in most studies on PFPS found in the literature,
it is only possible to make general comparisons. In order to further develop treatment models for PFPS we advocate prospective, randomised, controlled, long
term studies using validated outcome measures. However, there is a strong need
for basic research on the nature and aetiology of PFPS in order to better understand this mysterious syndrome.
1. Definition of Patellofemoral Pain
Syndrome (PFPS)
There is no clear consensus in the literature on
the terminology for pain in the anterior part of the
knee.[1] Patellofemoral pain syndrome (PFPS) is
difficult to define, as patients experience a variety
of symptoms from the patellofemoral joint with different levels of pain and physical impairment. The
terminology is thus still widely discussed. Anterior
knee pain, chondromalacia patella, patellofemoral
arthralgia, patellar pain, patellar pain syndrome and
patellofemoral pain are often used synonymously
with PFPS.[2,3]
Adis International Limited. All rights reserved.
The term anterior knee pain is suggested to
encompass all pain-related problems of the anterior
part of the knee.[3-5] By excluding anterior knee
pain due to intra-articular pathology, peripatellar
tendinitis or bursitis (table I), plica syndromes,
Sinding Larsens disease, Osgood Schlatters disease, neuromas and other rarely occurring pathologies it is suggested that remaining patients with a
clinical presentation of anterior knee pain could be
diagnosed with PFPS.[3,5] The term patellofemoral
seems appropriate, as no distinction can be made
as to which specific structure of the patella or the
femur is affected. Pain is the symptom that all
patients experience, but patients have other sympSports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
247
Table I. Pathologies that can generate anterior knee pain
Intra-articular pathology (including both the tibiofemoral and patellofemoral joint)
Peripatellar tendinitis or bursitis
Cartilage damage
Quadriceps tendinitis
Menisci, ligament and capsular damage
Patellar tendinitis
Sequelae after patellar fracture, dislocation or subluxation
Iliotibial band friction syndrome
Sequelae after knee surgery
Pre- and infrapatellar bursitis
Pes anserinus bursitis
toms as well, and thus it is appropriate to use the
word syndrome, defined as a group of signs and
symptoms that occur together and characterise a
particular abnormality.[6]
The term chondromalacia patellae, defined at
the beginning of the 20th century to describe pathological changes of the retropatellar cartilage,[7,8] was
for half a century, used as a synonym for the syndrome of patellofemoral pain. However, several
studies during the last 2 decades have shown a poor
correlation between articular cartilage damage and
the still not well-defined pain mechanism of retropatellar pain.[4,9-15]
2. The Patellofemoral Joint
2.1 Anatomy and Biomechanics
The patellofemoral joint consists of the patella,
the distal and anterior parts of the femur, articular
surfaces and surrounding supporting structures. The
patella is a sesamoid bone of relatively constant
length, width and thickness. Seventy-five percent
of the posterior surface of the patella is covered by
cartilage up to 5mm thick, making it the thickest in
the body. The patella increases the lever arm for
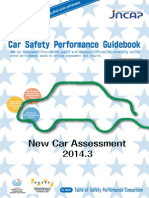
the quadriceps/patellar tendon by up to 50% and
also protects the anterior part of the knee joint (fig.
1).[2,16-18]
The patella is passively stabilised by the shape
of the patella, the trochlea of the femur and the
peripatellar retinaculum. The dynamic stabilisers
of the patella include the pes anserinus and semimembranosus muscles, rotating the tibia inward,
the biceps femoris muscle, rotating the tibia outward, the vastus medialis muscle, pulling the patella medially, the vastus lateralis (VL) muscle,
pulling laterally, and the vastus intermedius and
Adis International Limited. All rights reserved.
rectus femoris muscles, pulling proximally/laterally. The distal part of the vastus medialis, the vastus medialis obliquus (VMO) muscle, has its own
nerve supply and can pull the patella medially at a
knee angle of 65 (fig. 1).[2,16,17,20]
During extension from approximately 30 of
knee flexion, the tibia rotates outwards and the patella is guided through the trochlea of the femur by
the interacting heads of the quadriceps muscle. At
full knee extension, the patella rests on the suprapatellar fatpad/bursa. During knee flexion from full
knee extension, the distal part of the patella comes
in contact with the lateral femoral condyle at 10 to
20 of knee flexion, and the patella then follows an
S-shaped curve through the trochlea. The part of
the patellar surface articulating with the femur moves
proximally during flexion of the knee (fig. 1).[2,16-18]
Patellofemoral compression forces increase with
increasing knee angles up to 90 of knee flexion
and can reach up to 8 times bodyweight.[2]
2.2 Cartilage Properties
The cartilage has viscous and elastic properties,
i.e. a fluid component for force absorption and lubrication of the articular surface, and elasticity to
distribute and absorb forces. The cartilage, supported
by subchondral bone, is divided into 3 main layers.
The basal layer attaching to the subchondral bone,
with a perpendicular collagen orientation, is highly
efficient for force transfer and absorption. The second layer of collagen bundles is efficient in resisting shear and has high shock-absorbing qualities
owing to the high viscosity. The surface layer has
tangential-orientated collagen with very low friction, which facilitates motion (fig. 2). Nutrition to
the cartilage is supplied through diffusion from the
synovial fluid. Pressure changes the permeability
Sports Med 1999 Oct; 28 (4)
248
Thome et al.
Anterior superior
iliac spine
Q angle
Vastus
lateralis
30-40
Vastus
medialis
50
65
Vastus
medialis
obliquus
Centre of
patella
Tibial
tuberosity
90
45
Lateral
20
Medial
Among 15 year olds, the incidence was 10%. The
major symptoms were pain and crepitation in the
patellofemoral joint, especially during loading of
this joint and palpation of the patella. In addition,
pain while sitting and occasional weakness and
catching sensations were reported. The symptoms
often prohibited the students from participating in
school physical education, and recreational and
competitive sports. Fairbank et al.[23] studied 446
randomly-selected students aged 13 to 19 years.
The symptomatology was the same as in the study
by Hrding.[24] During the year prior to the study,
136 students (30%) had experienced anterior knee
pain. Of these 136 students, 25 had stopped participating in sports. No difference was found between
students with knee pain and those without, in terms
of joint mobility, Q angle, genu valgum and anteversion of the femoral neck.
4. Aetiology of PFPS
135
Fig. 1. The articular surfaces of the patellofemoral joint and patella. The Q angle and the angles of pull by the different parts
of the quadriceps muscle are illustrated on the left. Shaded
areas on the right indicate areas of articular contact on the patella with increasing knee flexion.[16-19]
of the cartilage, and synovial fluid diffuses into the
middle layer. A lubricating fluid is pressed out to
the articular surface, resulting in a nearly frictionless surface (fig. 2).[2,16,17]
3. Incidence of PFPS
Among injuries to physically active adolescents
and young adults, knee problems are one of the
most common, of which anterior knee pain is the
most frequent complaint. In reports from different
sports medicine clinics, knee problems account for
23 to 31% of injuries and complaints, where pain
conditions related to the patellofemoral joint are
the most common.[2,11,21-28] Hrding[24] reported that,
among 1990 students between the ages of 10 and
19 years, anterior knee pain was the most frequent
complaint and was seen in 3.3% of this group.
Adis International Limited. All rights reserved.
To assess the degree of PFPS, a variety of symptoms and different levels of pain and physical impairment must be considered. The aetiology is still
unclear in many patients. Three major contributing
factors increasing the risk of developing PFPS are
discussed: malalignment of the lower extremity
and/or the patella, muscular imbalance of the lower
extremity, and overactivity.[2-4,16,29,30]
4.1 Malalignment
4.1.1 Malalignment of the Lower Extremity
Malalignment of the lower extremity has been
considered a contributory factor in the development
of PFPS. Lower extremity alignment factors associated with patients with PFPS include femoral neck
anteversion, genu valgum, knee hyperextension, Q
angle, tibia varum and excessive rearfoot pronation.[2,31] However, clinical studies have not been
able to demonstrate biomechanical or alignment differences between patients with PFPS and healthy
individuals.[3,5,23,32,33] Fulkerson and Hungerford (in
Grayson[2]) did not find any direct correlation between a high Q angle and patellofemoral pain, an
opinion supported by others.[3,23,32-34] A high Q angle
may be a contributing factor in maintaining PFPS
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
once it has been acquired, but this is not very well
studied. However, Messier et al.[35] studied 36 male
and female runners between 16 and 50 years of age
and found that the Q angle was a discriminator between runners with PFPS and symptom-free runners.
Reid[3] questioned the use of the term malalignment and argued that 60 to 80% of the normal population falls into a category generally classified as
malalignment.
4.1.2 Patellar Malalignment
The shape of the patellar and femoral surfaces,
the configuration of the trochlea and the inter-relationship between these factors are often discussed. Three different patterns of patellar
malalignment have been described in the literature:
subluxation without tilting, subluxation with tilting, and tilting without subluxation.[36,37] However, no difference was found with computerised
tomography (CT) between the patients most
symptomatic and least symptomatic knees in a
study by Thome et al.,[5] and the values for patellar tilt angle, congruence angle and patellar subluxation were found to be within normal limits.[37-39]
These results are in contrast with those of Insall et
al.,[40] using radiographic examination, who stated
that patellar tracking abnormalities were the major
cause of patellar pain. The reason for the normal
CT values in the study by Thome et al.[5] was
probably that the patients had patellofemoral pain
only and no history or signs of patellar instability.
The significance of lower extremity alignment
factors and pathological limits thus needs further
investigation. It is possible that the definitions used
for malalignment should be re-evaluated as the scientific support is very weak with regard to determining when alignment is normal and when there
is malalignment. Pathological limits must be clarified. Various pathological limits are stated in the
literature, indicating that if the patient exceeds various lower limb alignment measurements, this will
predispose for PFPS or indicate certain surgical
procedures. Reid[3] stated that among all alignment
measurements found in the literature, only leg length
discrepancy (not supported by Thome et al.[5]) is
Adis International Limited. All rights reserved.
249
Advancing
load
Agitation and
normal diffusion
Surface layer
low friction
Middle layer
shock absorption
Basal layer
force transfer
and absorption
Subchondral bone
Fig. 2. Three main layers of the articular surface and effects of
loading on articular cartilage permeability. An advancing load
compresses the articular cartilage and causes an expulsion of
fluid. Decreased permeability is created in the area of compression with return of normal permeability behind the advancing
load (redrawn from James,[21] with permission).
consistently found to be a significant factor in the
aetiology of PFPS.
Alignment factors are largely measured in static
positions, and not during movement. However, in
a recent kinematic CT study of the patellofemoral
joint during active flexion and extension, lateral
patellar translation and tilting was detected in 8 of
20 knees with anterior pain.[41] Using high-speed
cinematography, Dillon et al.[42] found significant
differences in gait patterns between college aged
women with symptoms of anterior knee pain compared with those without symptoms. In another study
by Powers et al.,[43] volunteers with and without
PFPS underwent gait analysis (stride characteristics
and joint motion) during level and stair walking.
Compared with the comparison group, the primary
gait compensation in the PFPS group was a reduced
walking speed, which was a function of both stride
length and cadence. It cannot be excluded that the
dynamics of the patellofemoral joint result in a
higher risk for overuse of this joint in some individuals. Any combination of malalignment and
muscle function deficit would probably increase
this risk. If this reasoning holds true, investigations
should be performed with the aim of evaluating
how much malalignment and/or muscular function
Sports Med 1999 Oct; 28 (4)
250
deficit must be present in order to increase the risk
for overuse of the patellofemoral joint during physical activity to a certain degree.
4.2 Muscular Imbalance
Muscle tightness in the quadriceps or hamstrings
has been proposed as an important factor associated with knee extensor mechanism disorders.[44]
However, measurements of the range of motion of
the hip, knee and ankle joints have not demonstrated
any significant differences between patients with
PFPS and healthy individuals.[5,23] Muscular imbalance with decreased strength because of hypotrophy or inhibition of the lower extremity muscles
has been suggested as a potential cause of
PFPS.[2,16,21,29,30,45] However, whether decreased
strength is a cause or an effect of PFPS remains
undetermined.
Decreased knee extensor strength is a common
finding in patients with PFPS,[16,23,29,30,33,45-51] and
various patterns of weaknesses have been reported.
Bennett and Stauber,[46] Werner[51] and Thome et
al.[45] found selective weakness in eccentric muscle
strength. Quadriceps electromyogram (EMG) activity can be higher and less efficient in the painful
leg compared with the non-painful leg.[52] However, Mller et al.[53] and Thome et al.[45] found
that PFPS patients had lower EMG activity than
control patients during terminal maximal knee extension in the sitting position. Selective disturbances
within the quadriceps muscle have also been suggested.[54-61] Souza and Gross,[55] studying patients
with PFPS, and Voight and Wieder,[56] studying
patients with knee extensor mechanism disorders,
suggested that an abnormal relationship between
the VMO and VL muscle activation pattern can
disturb the dynamics of the patellofemoral joint.
Many exercise treatments emphasise the importance of the VMO because of its medial pull on the
patella.[62-65] However, Cerny[54] reported that neither exercises purported to selectively activate the
VMO muscle nor patellar taping improved the
VMO : VL ratio over similar exercises. Morrish and
Woledge,[60] and Witvrouw et al.[58] reported a
reversal of the onset of VMO and VL activity in
Adis International Limited. All rights reserved.
Thome et al.
patients with patellofemoral pain, where the reflex
response time of the VL was significantly shorter
than that of the VMO. In normal individuals, significant earlier firing was obtained from the VMO
compared with the VL. In contrast, Powers et al. [59]
found no differences in the onset or cessation of
muscle activity among the vastus muscles in patients
with PFPS.
Thome et al.[45] found that the EMG activity in
the vastus medialis muscle during both concentric
and eccentric knee extension was significantly lower
in the knee angle range of 25 to 50 than the range
of 50 to 75 for the patients most and least symptomatic knee. The explanation for lower strength
and EMG activity may be that patients with PFPS
have more symptoms and pain during the last 30
of maximal sitting knee extension compared with
the 90 to 30 range.[2,3,16,21] The results from vertical jump tests reinforce the results of the knee extension torque measurements, with significant differences observed between the patients and control
individuals in a unilateral drop jump from 20cm.[45]
The unilateral drop jump, with the whole body weight
on one leg and an eccentric/concentric movement
in the knee range close to full extension, places a
very high load on the patellofemoral joint.
Some studies showed that the quadriceps EMG
activity increases in normal individuals and in patients with anterior knee pain as the knee is extended.[53,66] However, Mariani and Caruso[67] reported decreased EMG activity of the vastus medialis
muscle among 8 patients with a history of patellar
subluxation during the last 30 of dynamic knee
extension for both the affected and the non-affected side. Others have found unchanged EMG
activity, or that the EMG activity was greatest at a
90 knee angle, but with great individual variation.[19,45,68] Methods of assessment, variations in
techniques, and differences in volunteers studied
may explain these differences in results.
The significance of muscle function in a closed
vs open kinetic chain has been discussed,[15,18,69-74] but
is far from well investigated. Hungerford and
Barry[18] showed that there was a significant difference in patellofemoral joint compression forces when
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
loading the patellofemoral joint during standing
(closed kinetic chain) compared with sitting (open
kinetic chain). Most strength measurements of patients were made in the sitting position, and it is
uncertain how valid these measurements are for
performance in the standing position. In a study on
muscular activation in the sitting and standing positions, with great care taken in standardising the
positions, a high reproducibility at repeated tests
could be demonstrated.[75] Both the patients and
the control group produced higher isometric knee
extensor torque per knee at a 60 knee angle at
1-legged muscular activation in sitting compared
with 2-legged muscular activation in standing positions. Furthermore, there was a high correlation
between sitting and standing torque measurements.
However, no difference was found between patients
with PFPS and healthy individuals in sitting or
standing knee extensor strength measurements.[75]
Differences in activation levels can be expected
between 1- and 2-legged muscular activation as a
result of a possible central nervous system limitation to maximally activate or control all synergistic
and antagonistic muscles, as demonstrated by Secher
et al.[76] In a study of 155 male and female, untrained and trained, healthy volunteers, they showed
that the 2-legged strength was 82% of the sum of
the strength in the right and left leg. The torque
during standing position in the study by Thome et
al.[75] was 82 and 68% of the sitting torque values
for the patients and control individuals, respectively.
Closed kinetic chain exercises appear to have
gained popularity over more traditionally used open
kinetic chain exercises because many clinicians
believe that closed kinetic chain exercises are safer
and more functional.[77,78] Therefore, the importance
of using closed kinetic chain rehabilitation[79-81]
and evaluation[82,83] has been stressed. Moreover,
a recent study[84] comparing the effect of closed
versus open kinetic chain exercises on strength and
performance showed larger improvements with the
closed kinetic chain group. However, it is clear that
both closed and open kinetic chain exercises can
be useful in a PFPS training programme to minimise
the risk of excessive patellofemoral joint stress.
Adis International Limited. All rights reserved.
251
Steinkamp et al.[85] described a mathematical model
for estimating patellofemoral joint stress during
closed and open kinetic chain exercise. Patellofemoral joint stress can be minimised or increased during both types of exercise, depending on the range
of motion through which the exercise is performed.
During the closed kinetic chain exercise, patellofemoral joint stress is steadily increased as the knee
is moved from an extended position to 90 of flexion.
In contrast, during the open kinetic chain exercise,
patellofemoral joint stress is steadily increased as
the knee is moved from 90 to full extension.
In summary, based on studies available, it is
clear that further studies are necessary in order to
establish the significance of various strength deficits and muscular imbalances and clarify if a specific disturbance in muscular activation is a cause
or effect (or both) of PFPS.
4.3 Overactivity
The importance of physical activity level and
overuse has been discussed in several studies, and
it appears that the stimulus for developing and exhibiting PFPS may be related to increased physical
activity and overloading rather than malalignment
of the patellofemoral joint.[3,5,23,32,33,35] Fairbank
et al.[23] found that patients with anterior knee pain
were significantly more involved in competitive
sports than age-matched control individuals selected
from the normal population, and that pain was associated with increased physical activity. Thome
et al.[5] found that: (i) all patients reported an insidious onset of symptoms associated with temporary
overuse or a period of increased physical activity;
(ii) the patients were significantly more involved
in competitive sports than the controls. This agrees
with the findings of Fairbank et al.;[23] (iii) the patients had a significantly lower pain-free activity
level[86] than the control individuals; (iv) when
specifically asked, all patients stated that both their
maximal level of pain and their average highest
level of daily pain, as measured with a visual analogue scale, was associated with increased physical
activity; and (v) patients with a high physical activity level did not experience more pain than those
Sports Med 1999 Oct; 28 (4)
252
with a low activity level. These findings indicate
that increasing the physical activity level too drastically might result in an increased risk for developing PFPS.[5]
5. Symptoms
The most common symptoms in patients with
PFPS are pain, complaints of crepitus, giving way
and catching, occasional sensations of stiffness and
sensations of swelling.[2,5,32] Crepitus experienced
in the patellofemoral joint while flexing and extending the knee is a common symptom. However,
crepitus is not always present in patients with PFPS
and can furthermore be present without any pain or
other symptoms. Swelling is rare and, when reported, is mild and intermittent.
Symptoms of giving way can occur in patients
with PFPS with a sudden relaxation due to pain
inhibition of the quadriceps muscle during loading
of the patellofemoral joint in standing. This should
be distinguished from giving way as a result of ligamentous instability of the knee joint or meniscal
lesion during a turning movement. Giving way and
sensations of catching may be misinterpreted in determining whether intra-articular pathology is
present in the tibio-femoral joint. Fulkerson and
Hungerford[2] stated that patients with intra-articular
pathology in the tibio-femoral joint most often experience giving way while turning, and that giving
way caused by a patellofemoral problem most frequently occurs during ascending stairs or walking
down an incline.[2,5]
Catching or a locking sensation is often reported,
but is primarily transient. The sensations of catching and locking experienced by patients with PFPS
should be carefully evaluated and distinguished from
catching and locking due to intra-articular pathology.[2,3]
Unfortunately, the documentation, evaluation and
analysis of the type, duration and intensity of pain
and common clinical symptoms in different activity
situations and levels for patients with PFPS are
scarce in the literature.
Adis International Limited. All rights reserved.
Thome et al.
5.1 Pain
Pain is a common symptom in many different
musculoskeletal disorders. There are several types
of clinical manifestations of pain (such as sharp,
dull, aching, throbbing, etc.), which is why a differentiated documentation of the patients pain
symptoms can be necessary.[87] The source of
patellofemoral pain in patients with PFPS cannot
be sufficiently explained. There are no nerve endings in the articular cartilage,[88] but pain can be
elicited from the innervated subchondral bone.[2,89]
A reactive synovial change can also be a possible
source of pain but, as effusion is uncommon,[5] and
mild when present, it is less likely that the pain
arises from the synovium.[3] Fulkerson et al.[90] discussed the patellar retinacula as a potential source
of patellofemoral pain, as they found histopathological evidence of degenerative neuropathy of the
lateral retinaculum in patients with patellofemoral
retinacular tightness. Increased physical activity
could result in peripatellar soft tissue irritation and
pain may then generate from retinacular nerve endings. It is possible that malalignment factors and
overactivity may magnify this effect.[2,3,5,91]
The most common symptom of PFPS is pain
during and after physical activity, during bodyweight
loading of lower extremities in walking up/down
stairs and squatting, and in sitting with the knees
flexed.[2,3,5,21,23,30,32,92] A Visual Analogue Scale
(VAS)[47,93] has been found to be both reliable and
valid for measuring pain.[94,95] The VAS, usually
presented as a 100mm-long line with the endphrases[96] no pain and pain as bad as it could
be, correlates well with verbal scales and numerical rating scales.[97] The VAS has been found to be
more satisfactory for patient self-rating of pain intensity than 3- to 5-point verbal scales.[93,98-100]
However, Carlsson[101] questioned the basis for
these claims and found that, despite practice, patients appeared to differ considerably in their ability to use the VAS. Harms-Ringdahl et al.[102]
showed the VAS to be as reliable in assessing intensity levels of perceived pain elicited by loading
joint structures as Borgs category scale (CR-10
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
scale) with ratio properties for intermodal and interindividual comparisons.[103]
The VAS scores, which in principle should be
viewed as data on an ordinal scale,[93,104] can be
transformed to an interval scale by using the Rasch
analysis.[105] This allows for analysis of the hierarchical order, which is of interest in understanding
different pain-provoking situations in relation to
pain assessment according to memory, and also
gives individual measurement values with errors
for testing changes in individual patients before
and after treatment. The Rasch analysis is based on
the patients ability and on the difficulty of the item
(test situation). In a study by Thome et al.,[106] the
patients ability was replaced by the patients pain
level. The item difficulty was replaced by the value
of the pain scores on the item. The items were correspondingly positioned along a measurement line
from the most to the least pain-provoking item.
Using the VAS, Thome et al.[106] could show that
it was possible to assess pain levels in different
pain-provoking situations (items) dealing with
memories of pain, pain provoked by various tests
and pain during physical activity. The different items
were hierarchically ordered in the Rasch analysis,
illustrating the relation of the items to each other.
It was then also possible to test the significance of
changes in individual patients during treatment and
identify patients with different recovery times.
However, among activity related items, such as
descending stairs, there was a lack of items for high
level pain assessment. It was suggested that additional items should be added, such as prolonged
sitting, running on stairs, running on hilly terrain
and 1-legged jumping, to fill this gap. At the low
end of the VAS, where patients who benefit from
treatment are found, there was a similar insufficiency of low pain-provoking items that would make
the measures of low levels of pain more precise.[106]
The Rasch analysis identifies patients who report
too much or too little pain on a certain item in relation to what they report on other items. This information on the so-called misfits can be useful in
the clinic, in combination with anamnestic and clinical findings, for increasing an understanding of the
Adis International Limited. All rights reserved.
253
patients symptomatology.[106] A vertical jump test
and a dynamic strength test showed the highest frequency of misfit VAS responses. These are items
in which relatively high loads are applied to the
patellofemoral joint.
Difficulties in standardising the jump test and
varying pain expectations among patients during
the maximal dynamic knee extensor strength test
may contribute to the high frequency of responses
deviating from what was expected by the Rasch
model. Other test items, such as walking up and
down stairs, a palpation test and a compression test
appeared to be more standardised.[106] The advantages and possibilities using the Rasch analysis for
further analysing VAS scores may be of great help
for a deeper understanding of PFPS, as well as other
pain syndromes caused by various musculoskeletal
disorders.[106]
5.1.1 Strength, Pain and Inhibition
Knee extensor strength deficit is a common finding
in patients with PFPS.[16,23,29,30,33,45-51] Thome et
al.[75] showed that patients with PFPS may have a
moderate reduction of maximal motor unit activation at maximal quadriceps effort as measured during knee extension in the sitting position. Extrapolation from several submaximal levels indicated
that an additional 18% (range 0 to 58%) of knee
extensor torque could be generated. Rutherford et
al.[107] found a great variation in lack of activation
(range 5 to 95%) among 6 patients with muscle
pain of various origins. Thome et al.[75] stated that
it is likely that the estimated additional torque that
could be generated at maximal effort among the
PFPS patients is a result of reflex inhibition caused
by afferent signals from the patellofemoral joint,
as the patients also reported pain during the strength
tests. A similar use of superimposed electrical
stimulation was reported by Lindh et al.[108] in patients with chronic muscular pain (fibromyalgia).
They did not report increased pain provoked by the
maximal sitting isometric knee extensor torque
measurements, and it was therefore suggested that
the inability for maximal activation was caused by
impaired control mechanisms at a spinal or supraspinal level. Whether this explanation may be appliSports Med 1999 Oct; 28 (4)
254
cable to the PFPS patients can neither be confirmed
nor excluded, although pain inhibition is likely to
occur in PFPS patients who report increasing pain
in isometric tests.
The decreased torque and reduction in EMG activity seen in patients with PFPS, especially during
eccentric knee extension, may imply quadriceps inhibition selective to heavy patellofemoral loading
such as eccentric knee extension and vertical jump
on one leg.[45,46,51] These effects seem to appear
specifically at knee angle ranges close to full extension and in the vastus medialis muscle.[45,53,55,109]
Inhibition and ability to develop torque in different
situations should be taken into account when developing treatment programmes for patients with
PFPS. Further studies should be performed to analyse the presence and impact of reflex inhibition.
5.1.2 Personality and Pain
With chronic pain as a dominant factor in PFPS,
greater attention has been focused on the relationship between personality and pain. Carlsson et al.[110]
discussed pain behaviour in patients with long term
PFPS and stated that chronic pain most often has a
multifactorial origin, and that the significance of
the psychosocial, social and biological factors may
vary. By observing the patients facial expressions,
posture, verbal expressions and pain reactions on
different provocation tests, information can be attained regarding pain behaviour. Certain pain
behaviours may be more likely to recur or persist
because of their effects, while others may occur
less frequently or less intensely because reinforcing events no longer occur. Improvement in the
pain experience may follow an improvement in
functional abilities and activities.[110-113] Carlsson
et al.[110] found only a few significant differences
between knee patients and control individuals using several methods assessing anxiety, depression,
helplessness, aggression, hostility, passive attitudes
and alexithymic characteristics.
If the patient behaves as though he or she experiences significant pain and there is an absence of
adequate physical findings that might account for
this pain, it is a frustrating situation for both the
clinician and the patient. The pain behaviour of the
Adis International Limited. All rights reserved.
Thome et al.
patient is sometimes presumed to stem from some
kind of personality, emotional or motivational difficulty. When that assumption is made, the clinician often thinks of the patients pain as not real,
or as exaggerated or malingered. The implication
is that the patient is not really suffering.[111,114]
This latter feeling is often made apparent to many
patients with PFPS, not only by clinicians but also
by parents, peers, teachers, etc.[5] The prevalence
of any personality, emotional or motivational problems among patients with PFPS is not well documented.
6. Treatment
Basic knowledge is lacking and no strong scientific evidence has been presented in the literature on
the nature and aetiology of PFPS. This could explain
why there are so many treatment protocols described
in the literature.[15,62,70,71,109,115-125] However, Arroll
et al.[124] found only 5 randomised controlled trials
in their extensive review on non-operative therapy
for PFPS, and concluded that there is little evidence
on which to base therapy. The number of patients
experiencing PFPS are numerous and decisions
still have to be made daily, throughout the world,
on how a treatment programme should be set up for
these patients. We suggest a comprehensive approach
that can account for the complexity that PFPS presents us with.
Shelton and Thigpen[121] argued for avoiding a
cookbook approach and advocated a biomechanical approach. Progression should be achieved without increasing symptoms. Key factors in a training
programme are: strength, flexibility, proprioception, endurance, functional training and a gradual
progression of the exercise load.[62,70,121,122,109]
Another important factor is compliance, stressed
by Yates and Grana,[126] who found at 15-month follow-up in 64 patients that 42 were non-compliant,
17 partially compliant and 5 compliant with the
prescribed exercise programme. Surgical treatment
is rarely indicated,[71,109,127-129] and the most frequently recommended treatment for PFPS is an exercise programme.[15,70,71,109,121] The natural
course of 48 patients with PFPS given information
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
and an isometric training programme, when followed up after a mean period of 11 years, was
found to be excellent or good in 85%.[34] This
agrees with the findings of other studies.[129,130]
However, the effects of an exercise programme for
PFPS are not well documented. Various results (50
to 100% success rate) are reported, as well as variability among studies in the diagnoses, physical activity level, gender and age of the patients.
The following studies, all with limited scientific
evidence, present a spectra of various treatment approaches. Kannus and Niittymki,[33] ONeill et
al.,[131] and Werner and Eriksson[122] studied male
and female patients with PFPS and reported good
results from an exercise programme, while others[11,46,70,132] studied patients with anterior knee
pain with different possible underlying diagnoses.[3]
The earliest study in the literature, by DeHaven et
al.,[11] presented a prospective analysis of 100 athletes with the clinical diagnosis of chondromalacia
patellae. Eighty-nine percent of the athletes were
able to return to athletics after a treatment programme
consisting of: (i) symptomatic control; (ii) a progressive resistance programme of isometric quadriceps and isotonic hamstrings exercises; (iii) a graduated running programme; and (iv) a maintenance
programme.
Hrding[24] treated 34 students between 8 and
19 years of age with isometric training for those
with moderate complaints and a soft brace for those
with more serious complaints. After 4 months, 50%
of the students were symptom free. In a study by
Bennett and Stauber,[46] all 41 patients recovered
their eccentric strength in 4 weeks using eccentric
isokinetic exercises. After a 12-week treatment programme for patients with chondromalacia patellae,
McMullen et al.[132] could not find any difference
between an isometric and an isokinetic exercise
programme. Both programmes demonstrated significant functional improvements over a control
group receiving no treatment. ONeill et al.[131] found
that 80% of patients with PFPS were improved at
a follow-up 12 to 16 months after an isometric
strengthening programme that included stretching
exercises. Doucette and Goble[70] had an 84% suc Adis International Limited. All rights reserved.
255
cess rate of pain-free patients after 8 weeks of an
individualised, comprehensive, 5-stage physical
therapy programme including stretching, and isometric and dynamic strengthening exercises in both
open and closed chains.
Werner and Eriksson[122] found a significant
improvement in patients with PFPS in maximal concentric and eccentric knee extensor torque after 8
weeks of isokinetic training. The measurements and
training were performed in the sitting (open kinetic
chain) position. Kannus and Niittymki[33] showed
complete recovery in 70% of patients with PFPS,
with a reduction of physical activity level by the
elimination of all symptom-producing activities,
enforcement of a quadriceps strengthening programme and the use of nonsteroidal anti-inflammatory medication. Stiene et al.[133] compared closed
kinetic chain and isokinetic joint isolation exercise
(open kinetic chain) in patients with patellofemoral dysfunction. They found that both groups had
significant improvement in an isokinetic knee extension test, but only the closed kinetic chain group
showed significant improvement in closed kinetic
chain testing and perceived functional status.
Thome[109] presented a successful comprehensive treatment approach for PFPS. The approach is
based on standardised information, a pain monitoring
system and an exercise programme with a progression plan allowing for the individually and specifically designed treatment approach advocated in
recent studies.[3,15,70,71,121,134-136] A significant reduction in pain and improvements in strength and
physical activity level were seen after 12 weeks of
treatment. Furthermore, all 40 patients had significantly less pain, as analysed with the Rasch analysis, at the 12-month follow-up compared with before
treatment. At the 12-month follow-up, 90% of the
patients were engaged in competitive or recreational
sports without pain and 39 patients, 2 of whom had
undergone surgery (lateral retinacular release), rated
their knee function as excellent or good. Reasons
for improvement may be an effect of time, the
standardised information, the pain monitoring system, the gradually progressive training programme
and the adjusted physical activity level. The study
Sports Med 1999 Oct; 28 (4)
256
lacked a proper control group receiving no treatment, which limits the possibilities for evaluating
the effects of treatment. However, the patients
were retrospectively their own controls, having an
average of 8 months of rest without relief of symptoms. Thus, time is not likely to be a major cause
of the improvement.
It is likely that the standardised information results in a better understanding of PFPS and that the
information given may have contributed to an altered physical activity pattern. The patients were
allowed to continue, using the pain monitoring system, with adjusted physical activity during treatment. This resulted, for example, in an avoidance
or reduction of temporary heavy loading of the
patellofemoral joint.
In the study by Thome,[109] no significant differences in physical activity levels, pain and muscle
function were found between the 2 training groups.
Thus, the treatment effects do not seem to be sensitive to a particular choice of exercise in the training
programme. A reduction in pain that lasted through
and for 1 to several hours after the training programme was reported by most patients after a 10 to
15 minutes of training. Thus, the author speculated
that the exercises used may have modified the inflow of afferent signals with reduced reflex inhibition and possible effects on the endorphin system.
Better muscle activation, with increased motor unit
recruitment as well as a more normal activation of
the vastus medialis muscle, may thus be achieved.
The training programme used by Thome[109]
might also result in an increased diffusion of nutrients to the cartilage caused by loading and unloading the patellofemoral joint,[21,135] and improved
nutrition to surrounding joint structures and muscles owing to increased blood circulation. Thus, it
may be anticipated that the training programme
yielded positive effects on the patellofemoral joint
structures, as adaptive changes can be seen in muscles, tendons, ligaments and the cartilage after regularly repeated, slowly progressing, non-strenuous
physical training.[124,137-140] However, this reasoning
is only speculative, with limited scientific support.
Exercises that are too strenuous or biomechanic Adis International Limited. All rights reserved.
Thome et al.
ally unfavourable may cause a gradual breakdown
of the musculoskeletal tissue, articular cartilage being the most sensitive of these,[138] which emphasises the need for a carefully controlled training
programme. The increased physical activity after
treatment may contribute to the further improvements in symptoms and muscle function seen at the
12-month follow-up.[109]
In this study, a pain monitoring system was used
allowing for pain evaluation and monitoring in
which pain during and after exercise or physical
activity was permitted. This is in contrast to recent
review articles on the treatment of patellofemoral
pain, which advocate that all training should be
done pain free.[3,121,134-136] Thome[109] argued that
it is likely that maintaining a level of no pain during
or after physical activity for patients with PFPS
requires such a decrease in physical activity and
loads during treatment that improvements may fail
to appear. However, the acceptance of a level of
pain that is too high can result in immediate and
frustrating setbacks. The pain monitoring system
used by Thome[109] allowed for gradual exercise
progress with minimal risks for overloading and
overuse of the patellofemoral joint. As patient
compliance was very high and there were no dropouts, use of the pain monitoring system is advocated in the treatment of patients with PFPS.[109]
6.1 Patellar Taping
The recommended approach to taping for patellar
malalignment cited in many recent articles[62] was
not considered in the study by Thome,[109] as the
patients in that study had no signs of patellar malalignment. A recent study[141] reported poor to fair
reliability among 12 physical therapists, comparing
a series of patellofemoral alignment tests to determine when and how patellofemoral taping techniques should be used. This was not surprising, as
patellar malalignment is a questionable characteristic
of PFPS.[3,5,23,32,33] Werner et al.[142] found that patients with patellar hypermobility increased their
knee extensor torque with taping. However, Cerny[54]
could not improve the EMG activity ratio between
the VMO and the VL muscles using patellar taping.
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
Positive effects of the McConnell[62] approach,
including taping and a functional lower extremity
exercise programme, might be found in factors discussed above and not necessarily be the result of
the specific taping techniques used. Kowall et
al.[143] evaluated the results of a physical therapy
programme that used patellar taping in a group of
patients with PFPS. These results were compared
with results from a similar group of patients who
underwent a physical therapy programme without
patellar taping, and suggested no beneficial effect
of adding a patellar taping programme to a standard physical therapy programme in the treatment
of patellofemoral pain. Using the McConnell[62]
medial glide patellar taping technique, Larsen et
al.[144] showed that taping was effective in significantly moving the patella medially, but that the tape
was ineffective in maintaining this significance
after exercise.
Gilleard et al.[61] investigated the effect of patellar taping on the onset of activity of VMO and
VL. Fourteen female patients with patellar pain
walked up and down stairs in 2 conditions: (i) with
the patellofemoral joint of the painful lower extremity taped so that the pain was reduced by at
least 50% on a pain provocation test; and (ii) without patellar taping. When the patellofemoral joint
was not taped, there was no difference in the onset
of activity between the VMO and VL during the
step-up and step-down tasks. In contrast, when the
patellofemoral joint was taped, the VMO was activated earlier than the VL during the step-up and
step-down tasks. The authors concluded that the
earlier activation of the VMO may alter the movement of the patella, and that further research is
needed to determine whether this occurs and
whether it is beneficial.
6.2 Surgical Treatment
Although non-operative treatment is always
preferable for PFPS as the primary treatment, more
than 100 surgical procedures have been described
for the treatment of patellofemoral disorders. Most
of these operations, rarely evaluated with randomised
controlled studies, are directed at treating malalign Adis International Limited. All rights reserved.
257
ment (often called realignment procedures) or other
abnormalities of the extensor mechanism, or aimed
at treating injured cartilage.
Lateral retinacular release. This procedure can
be performed alone or in combination with other
realignment procedures. The main surgical indications are: (i) excessive lateral compression syndrome
with tenderness and tightness of the lateral retinaculum, combined with lateral patellar tilt; (ii) patellofemoral osteoarthrosis with lateral patellar tilt; and
(iii) persistent patellofemoral pain combined with
a lateral traction osteophyte at the insertion of the
lateral retinaculum into the patella.[145] This procedure is not recommended for very young patients,
or for patients with advanced patellofemoral osteoarthrosis and normal patellar tracking. The results
after this procedure have been unpredictable, with
a reported rate of satisfactory results between 20
and 92% of patients.[146] Furthermore, biomechanical studies have not shown any effect of this
procedure on the patellofemoral contact area or the
muscular forces around the knee.[147]
Proximal realignment procedures. Several different techniques for proximal, soft tissue realignment have been described. The most common is a
modification of the technique described by Insall
et al.[148] These procedures are mainly indicated in
patients who: (i) are skeletally immature and have
a history of recurrent dislocations; (ii) are skeletally mature or immature and have an increased
congruence angle combined with patellofemoral
pain; and (iii) have dysplastic femoral trochlea and
poor medial patellar support of the VMO muscle,
causing recurrent patellar subluxations or dislocations. Even though satisfactory results have been
reported in 79 to 91% of patients, these procedures
are now rarely used.[149]
Distal realignment procedures. These procedures
are most commonly used for recurrent patellar subluxation or dislocation and less for patellofemoral
pain. Several modifications of tibial tubercle transfer have been described. The indications for these
procedures are; (i) persistent patellofemoral pain
combined with excessive patellar tilt or subluxation or increased congruence angle; (ii) lateral
Sports Med 1999 Oct; 28 (4)
258
facet osteoarthrosis combined with a high Q angle;
and (iii) failed lateral release procedure, especially
in patients with significant lateral tilt or subluxation. This procedure should never be performed in
skeletally immature patients, because of a risk of
development of genu recurvatum.[150] Satisfactory
results have been reported in 80 to 96% of patients
after different distal realignment procedures.[151]
However, concerns have been raised about the long
term results.
Elevation of the tibial tubercle. Biomechanical
studies have shown a 50 to 83% decrease of patellofemoral compression force after elevation of the
tibial tubercle of 1.2 to 2.5cm.[152,153] The main indication for this procedure is moderate chondromalacia patellae (degeneration of the cartilage) or
osteoarthrosis that does not respond to non-surgical
treatment. Satisfactory clinical results have been
reported in 30 to 95% of patients treated with this
procedure,[154] and complications in 18 to 40%. As
the results have been very unpredictable and the
long term results unsatisfactory, this procedure is
now rarely used for patellofemoral pain.[155]
Anteromedial tibial tubercle transfer and elevation. This procedure has been advocated by Fulkerson[156] for patients with malalignment, an increased
Q angle, and mild-to-moderate osteoarthrosis. The
results have been reported as satisfactory in 75%
of patients after 5 years.[156]
Articular cartilage procedures. These procedures
include open or arthroscopic patellar shaving, local
excision of defects with drilling of the subchondral
bone, facetectomy and transplantation of autologous
chondrocytes. The major benefit of arthroscopic
interventions might be the lavage with removal of
debris from the knee joint. Local excision of diseased cartilage and subchondral drilling has been
used very commonly, even in patients with severe
chondromalacia of the patella. Satisfactory results
are achieved in several patients, especially below
the age of 25 years.[157] No comparative studies on
these procedures are available and the results are
often considered to be satisfactory in the short term,
but less is known about the long term outcomes.
Adis International Limited. All rights reserved.
Thome et al.
Patellectomy. This should be considered as the
last resort for treating patellofemoral diseases as it
often results in a considerable decrease in functional ability. The main indication for patellectomy
is severe patellofemoral pain after failed realignment procedure in a patient younger than 40 years.
Contraindications are tibial-femoral disorders and
patellofemoral pain of unknown cause.[158]
7. Conclusion
When individuals remain disabled for long periods despite a variety of treatments, and when the
disability diminishes when a new method is tried,
the inference can be drawn that the new treatment
is more effective. However, it may be difficult to
determine what the active ingredients are in a
complex treatment programme. Thome[109] argued
that the reasons for improvement with the comprehensive treatment approach used may be found in
the standardised information given, the pain monitoring system, the specified gradually progressing
training programme and adjusted physical activity.
PFPS is multifactorial, and thus it is likely that all
of the abovementioned reasons are active ingredients.
It seems most likely that standardised information and adjusted physical activity will be sufficient
for many PFPS patients having mild symptoms.
Avoiding abuse of the knee, avoiding pain-causing
activities such as heavy loading of the patellofemoral
joint, i.e. excessive stair walking or squatting, and
avoiding prolonged sitting with knees flexed could
be recommended. However, there is no reason why
patients with PFPS should give up their physical
activity. On the contrary, adjusted physical activity
seems important. For patients who have had PFPS
for more than 6 months, a detailed, specified training programme using a pain monitoring system
could be recommended.[109]
Another key word in the treatment of patients
with PFPS is patience. Improvements come slowly,
especially at the beginning of the treatment period,
and the positive effects of training on musculoskeletal tissue take time. It seems important that the
training programme gradually progresses in load
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
and the exercises used. The success of the treatment can also depend on the therapists ability to
adjust the various exercises of the training programme in relation to the patients specific symptoms and needs.
It is strongly suggested that, when presenting
reports on PFPS, a detailed description should be
provided of the diagnosis, individuals studied (inclusion and exclusion criteria), and methods in order to understand the conclusions drawn and be
able to compare results with other studies. As this
is not the case in most studies on PFPS found in
the literature, it is only possible to make general
comparisons. In order to further develop treatment
models for PFPS we advocate prospective, randomised, controlled, long term studies using validated
outcome measures. However, there is a strong need
for basic research on the nature and aetiology of
PFPS in order to better understand this interesting
syndrome.
References
1. Cutbill JW, Ladly KO, Bray RC, et al. Anterior knee pain: a
review. Clin J Sport Med 1997; 7: 40-5
2. Grayson TH, editor. Disorders of the patellofemoral joint. 2nd
ed. Baltimore (MD): Williams & Wilkins, 1990
3. Reid DC. The myth, mystic and frustration of anterior knee
pain. Clin J Sport Med 1993; 3: 139-43
4. Insall JN. Current concepts review: patellar pain. J Bone Joint
Surg Am 1982; 64 (1): 147-52
5. Thome R, Renstrm P, Karlsson J, et al. Patellofemoral pain
syndrome in young women: I. A clinical analysis of alignment, common symptoms and functional activity level. Scand
J Med Sci Sports 1995; 5: 237-44
6. Websters seventh new collegiate dictionary. Springfield
(MA): GC Merriam Co., 1969
7. Aleman O. Chondromalacia post-traumatica patellae. Acta Chir
Scand 1928; 63: 149-63
8. Bdinger K. Uber traumatische knorpelrisse in kniegeleuk.
Dtsch Z Chir 1908; 92: 510
9. Abernethy P, Wilson G, Logan P. Strength and power assessment. Sports Med 1995; 19: 401-17
10. Darracott J, Vernon-Roberts B. The bony changes in chondromalacia patellae. Rheum Phys Med 1971; 11: 175-9
11. DeHaven KE, Dolan WA, Mayer PJ. Chondromalacia patellae
in athletes. Am J Sports Med 1979; 7: 5-11
12. Hvid I, Andersen LI. The quadriceps angle and its relation to
femoral torsion. Acta Orthop Scand 1982; 53: 577-9
13. Kelly MA, Insall JN. Historical perspectives of chondromalacia
patellae. Orthop Clin North Am 1992; 23: 517-21
14. Leslie IJ, Bentley G. Arthroscopy in the diagnosis of chondromalacia patellae. Ann Rheum Dis 1978; 37: 540-7
15. Tria AJ, Palumbo RC, Alicea JA. Conservative care for patellofemoral pain. Orthop Clin North Am 1992; 23: 545-54
Adis International Limited. All rights reserved.
259
16. Ficat R, Hungerford D. Disorders of the patello-femoral joint.
Baltimore (MD): Williams & Wilkins, 1977
17. Hughston JC, Walsh WM, Puddu G. Patellar subluxation and
dislocation. Philadelphia (PA): WB Saunders, 1984
18. Hungerford DS, Barry M. Biomechanics of the patellofemoral
joint. Clin Orthop 1979; 144: 9-15
19. Lieb FJ, Perry J. Quadriceps function. An electromyographic
study under isometric conditions. J Bone Joint Surg Am 1971;
53 (4): 749-58
20. Reynolds L, Levin TA, Medieros JM, et al. EMG activity of the
vastus medialis oblique and the vastus lateralis in their role
in patellar alignment. Am J Phys Med 1983; 62: 61-70
21. James S. Chondromalacia of the patella in the adolescent. In:
Kennedy JC, editor. The injured adolescent knee. Baltimore
(MD): Williams & Wilkins, 1979: 205-251
22. Clement DB, Taunton JE, Smart GW, et al. A survey of running
injuries. Phys Sports Med 1981; 9: 47-58
23. Fairbank JC, Pynsent PB, van Poortvliet JA, et al. Mechanical
factors in the incidence of knee pain in adolescents and young
adults. J Bone Joint Surg Br 1984; 66 (5): 685-93
24. Hrding G. Chondromalacia patellae bland skolungdom. Nord
Med 1983; 98: 207-8
25. Kannus P, Aho H, Jrvinen M. Computerized recording of visits to an outpatients sports clinic. Am J Sports Med 1987; 15:
79-85
26. Kujala UM, Kvist M, sterman K. Knee injuries in athletes:
review of exertion injuries and retrospective study of outpatient sports clinical material. Sports Med 1986; 3: 447-60
27. Newman P, Thomson J, Barnes J, et al. A clinic for athletic
injuries. Proc R Soc Med 1969; 62: 939-41
28. Orava S. Exertion injuries due to sports and physical exercise:
a clinical and statistical study of nontraumatic overuse injuries
of the musculoskeletal system of athletes and keep-fit athletes
[thesis]. Oulo: University of Oulo, 1980
29. Bentley G, Dowd G. Current concepts of etiology and treatment
of chondromalacia patellae. Clin Orthop Rel Res 1984; 189:
209-28
30. Kujala UM, sterman K, Kvist M, et al. Factors predisposing
to patellar chondropathy and patellar apecitis in athletes. Int
Orthop 1986; 10: 195-200
31. Klingman RE, Liaos S, Hardin K. The effect of subtalar joint
posting on patellar glide position in subjects with excessive
rearfoot pronation. J Orthop Sports Phys Ther 1997; 25 (3):
185-91
32. Galanty HL, Matthews C, Hergenroeder AC. Anterior knee
pain in adolescents. Clin J Sports Med 1994; 4: 176-81
33. Kannus P, Niittymki S. Which factors predict outcome in the
nonoperative treatment of patellofemoral pain syndrome? A
prospective follow-up study. Med Sci Sports Exerc 1994; 26:
289-96
34. Karlsson J, Thome R, Swrd L. Eleven year follow-up of patellofemoral pain syndrome. Clin J Sports Med 1996; 6: 22-6
35. Messier SP, Davis SE, Curl WW, et al. Etiologic factors associated with patellofemoral pain in runners. Med Sci Sports
Exerc 1991; 23: 1008-15
36. Schutzer SF, Ramsby GR, Fulkerson JP. The evaluation of
patello-femoral pain using computerised tomography: a preliminary study. Clin Orthop 1984; 204: 186-293
37. Schutzer SF, Ramsby GR, Fulkerson JP. Computed tomographic
classification of patello-femoral pain patients. Orthop Clin
North Am 1986; 17: 235-48
38. Merchant AC, Mercer RL, Jacobsen RH, et al. Roentgenographic
analysis of patello-femoral congruence. J Bone Joint Surg
Am 1974; 56 (7): 1391-6
Sports Med 1999 Oct; 28 (4)
260
39. Stanford W, Phelan J, Kathol MH, et al. Patello-femoral joint
motion: evaluation by ultrafast computed tomography. Skeletal
Radiol 1988; 17: 487-92
40. Insall JN, Aglietti P, Tria AJ. Patellar pain and incongruence II:
clinical application. Clin Orthop 1983; 176: 225-32
41. Dupuy DE, Hangen DH, Zachazewski JE, et al. Kinematic CT
of the patellofemoral joint. Am J Roentgenol 1997; 169 (1):
211-5
42. Dillon PZ, Updyke WF, Allen WC. Gait analysis with reference
to chondromalacia patellae. J Orthop Sports Phys Ther 1983;
5: 127-31
43. Powers CM, Perry J, Hsu A, et al. Are patellofemoral pain and
quadriceps femoris muscle torque associated with locomotor
function? Phys Ther 1997; 77 (10): 1063-75
44. Antich TJ, Randall C, Westbrook RA, et al. Evaluation of knee
extensor mechanism disorders: clinical presentation of 112
patients. J Orthop Sports Phys Ther 1986; 8: 248-54
45. Thome R, Renstrm P, Karlsson J, et al. Patellofemoral pain
syndrome in young women: II. Muscle function in patients
and healthy controls. Scand J Med Sci Sports 1995; 5: 245-51
46. Bennett JG, Stauber WT. Evaluation and treatment of anterior
knee pain using eccentric exercise. Med Sci Sports Excerc
1986; 18 (5): 526-30
47. Campbell DE, Glenn W. Rehabilitation of knee flexor and knee
extensor muscle strength in patients with meniscectomies, ligamentous repairs, and chondromalacia. Phys Ther 1982; 62: 10-5
48. Dvir Z, Halperin N. Patellofemoral pain syndrome: a preliminary model for analysis and interpretation of isokinetic and
pain parameters. Clin Biomech 1992; 7: 240-6
49. Hoke B, Howell D, Stack M. The relationship between isokinetic
testing and dynamic patellofemoral compression. J Orthop
Sports Phys Ther 1983; 4: 150-3
50. MacIntyre D, Robertson G. Quadriceps muscle activity in women
runners with and without patellofemoral pain syndrome. Arch
Phys Med Rehabil 1992; 73: 10-4
51. Werner S. An evaluation of knee extensor and knee flexor torques
and EMGs in patients with patello-femoral pain syndrome in
comparison with matched controls. Knee Surg Sports Traumatol
Arthrosc 1995; 3 (2): 89-94
52. Doxey GE, Eisenman P. The influence of patellofemoral pain
on electromyographic activity during submaximal isometric
contractions. J Orthop Sports Phys Ther 1984; 9: 211-6
53. Mller BN, Krebs B, Tideman-Dal C, et al. Isometric contractions
in the patellofemoral pain syndrome: an electromyographic
study. Arch Orthop Traum Surg 1986; 105: 24-7
54. Cerny K. Vastus medialis oblique/vastus lateralis muscle activity
ratios for selected exercises in persons with and without
patellofemoral pain syndrome. Phys Ther 1995; 75 (8): 672-83
55. Souza DR, Gross MT. Comparison of vastus medialis obliquus:
vastus lateralis muscle integrated electromyographic ratios
between healthy subjects and patients with patellofemoral pain.
Phys Ther 1991; 71: 310-20
56. Voight ML, Wieder DL. Comparative reflex response time of
vastus medialis obliquus and vastus lateralis in normal subjects
and subjects with extensor mechanism dysfunction. Am J
Sports Med 1991; 19: 131-7
57. Boucher J, King M, Lefebvre R, et al. Quadriceps femoris muscle
activity in patellofemoral pain syndrome. Am J Sports Med
1992; 20: 527-32
58. Witvrouw E, Sneyers C, Lysens R, et al. Reflex response times
of vastus medialis oblique and vastus lateralis in normal subjects
and in subjects with patellofemoral pain syndrome. J Orthop
Sports Phys Ther 1996; 24 (3): 160-5
Adis International Limited. All rights reserved.
Thome et al.
59. Powers CM, Landel R, Perry J. Timing and intensity of vastus
muscle activity during functional activities in subjects with
and without patellofemoral pain. Phys Ther 1996; 76 (9): 946-55
60. Morrish GM, Woledge RC. A comparison of the activation of
muscles moving the patella in normal subjects and in patients
with chronic patellofemoral problems. Scand J Rehabil Med
1997; 29 (1): 43-8
61. Gilleard W, McConnell J, Parsons D. The effect of patellar taping
on the onset of vastus medialis obliquus and vastus lateralis
muscle activity in persons with patellofemoral pain. Phys Ther
1998; 78 (1): 25-32
62. McConnell J. The management of chondromalacia patellae: a
long term solution. Aust J Phys Ther 1986; 32: 215-23
63. Hehne HJ. Biomechanics of the patellofemoral joint and its clinical relevance. Clin Orthop 1990; 258: 73-85
64. Grabiner MD, Koh TJ, Miller GF. Fatigue rates of vastus medialis
oblique and vastus lateralis during static and dynamic knee
extension. J Orthop Res 1991; 9: 391-7
65. Weinstabl R, Schaf W, Firas W. The extensor apparatus of the
knee joint and its peripheral vasti: anatomic investigation and
clinical relevance. Surg Radiol Anat 1989; 11: 17-22
66. Speakman H, Weisberg J. The vastus medialis controversy.
Phys Ther 1977; 63: 279-83
67. Mariani PP, Caruso I. An electromyographic investigation of
subluxation of the patella. J Bone Joint Surg Br 1979; 61 (2):
169-71
68. Stratford P. Electromyography of the quadriceps femoris muscle
in subjects with normal knees and acutely effused knees. Phys
Ther 1981; 62: 279-83
69. Doucette SA, Child DD. The effect of open and closed chain
exercise and knee joint position on lateral patellar compression
syndrome. J Orthop Sports Phys Ther 1996; 23 (2): 104-10
70. Doucette SA, Goble EM. The effect of exercise on patellar
tracking in lateral patellar compression syndrome. Am J
Sports Med 1992; 20: 434-40
71. Zappala FG, Taffel CB, Scuderi GR. Rehabilitation of the patellofemoral joint disorders. Orthop Clin North Am 1992; 23: 555-66
72. Palmitier R, An K-N, Scott S, et al. Kinetic chain exercise in
knee rehabilitation. Sports Med 1991; 11 (6): 402-13
73. Beynnon B, Johnson R, Fleming B, et al. The strain behaviour
of the anterior cruciate ligament during squatting and active
flexion-extension. Am J Sports Med 1997; 25 (6): 823-9
74. Fitzgerald GK. Open versus closed kinetic chain exercise: issues
in rehabilitation after anterior cruciate ligament reconstructive
surgery. Phys Ther 1997; 77 (12): 1747-54
75. Thome R, Grimby G, Svantesson U, et al. Quadriceps muscle
performance in sitting and standing in young women with
patellofemoral pain syndrome and healthy controls. Scand J
Med Sci Sports 1996; 6 (4): 233-41
76. Secher NH, Rube N, Elers J. Strength of two- and one-legged
extension in man. Acta Physiol Scand 1988; 134: 333-9
77. Bynum BE, Barrack RL, Alexander AH. Open versus closed
chain kinetic exercises after anterior cruciate ligament reconstruction. Am J Sports Med 1995; 23: 401-6
78. Shelbourne KD, Nitz P. Accelerated rehabilitation after anterior
cruciate ligament reconstruction. J Orthop Sports Phys Ther
1992; 15: 256-64
79. De Carlo M, Shelbourne D, McCarroll J, et al. Traditional versus
accelerated rehabilitation following ACL reconstruction: a
one-year follow-up. J Orthop Sports Phys Ther 1992; 6: 309-16
80. Shelbourne K, Klootwyk T, Wilckens J, et al. Ligament stability
two to six years after anterior cruciate ligament reconstruction
with autogenous patellar tendon graft and participation in accelerated rehabilitation program. Am J Sports Med 1995; 5: 575-9
Sports Med 1999 Oct; 28 (4)
Patellofemoral Pain Syndrome
81. Callaghan MJ, Oldham JA. The role of quadriceps exercise in
the treatment of patellofemoral pain syndrome. Sports Med
1996; 21: 384-91
82. Greenberger H, Paterno M. Relationship of knee extensor strength
and hopping test performance in the assessment of lower extremity function. J Orthop Sports Phys Ther 1995; 5: 202-6
83. Wilk K, Romaniello W, Soscia S, et al. The relationship between
subjective knee scores, isokinetic testing, and functional testing
in the ACL-reconstructed knee. J Orthop Sports Phys Ther
1994; 2: 60-72
84. Augustsson J, Esko A, Thome R, et al. Weight training of the
thigh muscles using closed vs open kinetic chain exercises: a
comparison of performance enhancement. J Orthop Sports
Phys Ther 1998; 27 (1): 3-8
85. Steinkamp LA, Dillingham MF, Markel MD, et al. Biomechanical
considerations in patellofemoral joint rehabilitation. Am J
Sports Med 1993; 21 (3): 438-44
86. Tegner Y. Cruciate ligament injuries in the knee: evaluation and
rehabilitation [thesis]. Linkping: Linkping University, 1985
87. Lindblom U, Nmeth G. Smrttyper med eftersatt differentialdiagnostik. Lkartidningen 1992; 89: 1392-9
88. Biedert RM, Stauffer E, Friedrich N. Occurrence of free nerve
endings in the soft tissue of the knee joint: a histologic investigation. Am J Sports Med 1992; 20: 430-3
89. Kennedy JC, Alexander IJ, Hayes KC. Nerve supply of the
human knee and its functional importance. Am J Sports Med
1982; 10: 329-35
90. Fulkerson JP, Tenant R, Jiving JS, et al. Histologic evidence of
retinacular nerve injury. Clin Orthop Rel Res 1985; 197: 195-205
91. Goodfellow J, Hungerford DS, Woods C. Patello-femoral joint
mechanics and pathology. 2: chondromalacia patellae. J Bone
J Surg Br 1976; 58 (3): 291-9
92. Werner S, Eriksson E. Isokinetic quadriceps training in patients
with patellofemoral pain syndrome. Knee Surg Sports
Traumatol Arthrosc 1993; 1: 162-8
93. Scott J, Huskisson EC. Graphic representation of pain. Pain
1976; 6: 175-84
94. Dixon JS, Bird HA. Reproducibility along a 10 cm vertical
visual analogue scale. Ann Rheum Dis 1981; 40: 887-9
95. Price DD, McGrath PA, Rafii A, et al. The validation of visual
analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983; 17 (1): 45-56
96. Seymour RA, Simpson JM, Charlton JE, et al. An evaluation of
length and end-phrase of visual analogue scales in dental pain.
Pain 1985; 21: 177-85
97. Downie WW, Leatham PA, Rhind VM, et al. Studies with pain
rating scales. Ann Rheum Dis 1978; 37: 378-81
98. Joyce CRB, Zutshi DW, Hrubes V, et al. Comparison of fixed
interval and visual analogue scales for rating chronic pain.
Eur J Clin Pharmacol 1975; 8: 415-20
99. Kremer E, Atkinson JH, Ignelzi RJ. Measurement of pain: patient
preference does not confound pain measurement. Pain 1981;
10 (2): 241-8
100. Ohnhaus E, Adler R. Methodological problems in the measurement of pain: a comparison between the verbal rating scale
and the visual analogue scale. Pain 1975; 1: 379-84
101. Carlsson AM. Assessment of chronic pain. 1: aspects of the
reliability and validity of the visual analog scale. Pain 1983;
16 (1): 87-101
102. Harms-Ringdahl K, Carlsson AM, Ekholm J, et al. Pain assessment with different intensity scales in response to loading of
joint structures. Pain 1986; 27: 401-11
103. Borg G. A category scale with ratio properties for inter modal
and inter individual comparisons. In: Geisler HG, Petzold P,
Adis International Limited. All rights reserved.
261
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
editors. Psychophysical judgement and the process of perception. Berlin: VEB Deutscher Verlag der Wissenschaften, 1982:
25-34
Chapman SL, Casey KL, Dubner R, et al. Pain measurement:
an overview. Pain 1985; 22: 1-31
Wright BD, Stone MH. Best test design: Rasch measurements.
Chicago: Mesa Press, 1979
Thome R, Grimby G, Wright BD, et al. Rasch analysis of
visual analog scale measurements before and after treatment
of patients with patellofemoral pain syndrome. Scand J Rehabil
Med 1995; 27: 145-51
Rutherford OM, Jones DA, Newham DJ. Clinical and experimental application of the percutaneous twitch superimposition
technique for the study of the human muscle activation. J
Neurol 1986; 49: 1288-91
Lindh MH, Johansson LG, Hedberg M, et al. Studies on maximal voluntary muscle contraction in patients with fibromyalgia.
Arch Phys Med Rehabil 1995; 75: 1217-22
Thome R. A comprehensive treatment approach for patellofemoral pain syndrome in young women. Phys Ther 1997; 77
(12): 1690-703
Carlsson AM, Werner S, Mattlar C-E, et al. Personality in patients
with long term patello-femoral pain syndrome. Knee Surg
Sports Traumatol Arthrosc 1993; 1 (3-4): 178-83
Fordyce WE. Behavioral factors in pain. Neurosurg Clin 1991;
2: 749-59
Lindstrm IL. A successful intervention program for patients
with subacute low back pain [thesis]. Gteborg: Gteborg
University, 1994
Schwarz C, Blazina ME, Sisto DJ, et al. The results of operative
treatment of osteochondritis dissecans of the patella. Am J
Sports Med 1988; 16: 522-9
Sontag S. Illness as metaphor. New York (NY): Vintage, 1977
Eng JJ, Pierrynowski MR. Evaluation of soft foot orthotics in
the treatment of patellofemoral pain syndrome. Phys Ther
1993; 73: 62-70
Fisher RL. Conservative treatment of patello-femoral pain. Orthop Clin North Am 1986; 17: 269-72
Lindberg U. The patellofemoral pain syndrome [thesis].
Linkping: Linkping University, 1986
Lysholm J, Nordin M, Ekstrand J, et al. The effect of a patella
brace on the performance in knee extension strength test in
patients with patellar pain. Am J Sports Med 1984; 12: 110-2
Malek MM, Mangine RE. Patello-femoral pain syndrome: a
comprehensive and conservative approach. J Orthop Sports
Phys Ther 1981; 2: 108-16
Radin EL. A rational approach to the treatment of patello-femoral
pain. Clin Orthop 1979; 144: 107-9
Shelton GL, Thigpen LK. Rehabilitation of patellofemoral dysfunction: a review of literature. J Orthop Sports Phys Ther
1991; 14: 243-9
Werner S, Eriksson E. Isokinetic quadriceps training in patients
with patellofemoral pain syndrome. Knee Surg Sports
Traumatol Arthrosc 1993; 1: 162-8
Whitelaw GP, Rullo DJ, Markowitz HD, et al. A conservative
approach to anterior knee pain. Clin Orthop 1989; 246: 234-7
Arroll B, Ellis-Pegler E, Edwards A, et al. Patellofemoral pain
syndrome: a critical review of the clinical trials on nonoperative
therapy. Am J Sports Med 1997; 20: 207-12
Wise HH, Fiebert JM, Kates JL. EMG biofeedback treatment
for patellofemoral pain syndrome. J Orthop Sports Phys Ther
1984; 6: 95-103
Yates C, Grana WA. Patellofemoral pain: a prospective study.
Orthopaedics 1986; 9: 663-7
Sports Med 1999 Oct; 28 (4)
262
127. Evans TK, Paulos LE. Complications of patello-femoral surgery.
Orthop Clin North Am 1992; 23: 697-710
128. Karlsson J, Lansinger O, Swrd L. Bad results after anterior
advancement of the tibial tuberosity for patellofemoral pain
syndrome. Arch Orthop Trauma Surg 1992; 111: 99-104
129. Sandow MJ, Goodfellow JW. The natural history of anterior
knee pain in adolescents. J Bone Joint Surg Br 1985; 67 (1): 36-8
130. Jensen DB, Albrektsen SB. The natural history of chondromalacia
patellae: a 12 year follow-up. Acta Orthop Belg 1990; 56: 503-6
131. ONeill DB, Micheili LJ, Warner JP. Patellofemoral stress: a
prospective analysis of exercise treatment in adolescents and
adults. Am J Sports Med 1992; 20: 151-6
132. McMullen W, Roncarati A, Koval P. Static and isokinetic treatments of chondromalacia patella: a comparative investigation. J
Orthop Sports Phys Ther 1990; 12: 256-66
133. Stiene HA, Brosky, T, Reinking M, et al. A comparison of
closed kinetic chain and isokinetic joint isolation exercise in
patients with patellofemoral dysfunction. J Orthop Sports
Phys Ther 1996; 24 (3): 136-41
134. Beckman M, Craig R, Lehman RC. Rehabilitation of the patellofemoral dysfunction in the athlete. Clin Sports Med 1989; 8:
841-60
135. Brunet ME, Stewart GW. Patellofemoral rehabilitation. Clin
Sports Med 1989; 8: 319-29
136. Gray D. Physical therapy techniques for conservative treatment
of patellar pain and instability. Adapt Techn Sports Med
1994; 2: 263-72
137. Curtiss PH. Changes produced in the synovial membrane and
synovial fluid by disease. J Bone Joint Surg Am 1964; 46:
873-88
138. Kannus P, Jozsa L, Renstrm P, et al. The effects of training,
immobilization and remobilization on musculoskeletal tissue.
1: training and immobilization. Scand J Med Sci Sports 1992;
2: 100-18
139. Paukkonen K, Selkinaho K, Jurvelin J, et al. Cells and nuclei
of articular cartilage chondrocytes in young rabbits enlarged
after nonstrenuous exercise. J Anat 1985; 142: 13-20
140. Radin EL. The physiology and degeneration of joints. Semin
Arthritis Rheum 1973; 2: 245-57
141. Fitzgerald GK, McClure PW. Reliability of measurements obtained with four tests for patellofemoral alignment. Phys Ther
1995; 75: 84-92
142. Werner S, Knutsson E, Eriksson E. The effect of taping the patella
on concentric and eccentric torque and emg of knee extensor and
knee flexor muscles in patients with patello-femoral pain syndrome. Knee Surg Sports Traumatol Arthrosc 1993; 1: 169-77
143. Kowall MG, Kolk G, Nuber G, et al. Patellar taping in the treatment of patellofemoral pain: a prospective randomized study.
Am J Sports Med 1996; 24 (1): 61-6
Adis International Limited. All rights reserved.
Thome et al.
144. Larsen B, Andreasen E, Urfer A, et al. Patellar taping: a radiographic examination of the medial glide technique. Am J Sports
Med 1995; 23 (4): 465-71
145. Fulkerson, JP, Schutzer SF. After failure of conservative treatment for painful patello-femoral malalignment: lateral release
or realignment? Orthop Clin North Am 1986; 17: 283-8
146. Fabbriciani C, Panni AS, Delcogliano A. Role of arthroscopic
lateral release in the treatment of patello-femoral disorders.
Arthroscopy 1992; 8: 531-6
147. Hayes WC, Huberti HH, Lewallen DG, et al. Patellofemoral
contact pressures and the effects of surgical reconstructive
procedures. In: Ewing JW, editor. Articular cartilage and knee
joint function: basic science and arthroscopy. New York
(NY): Raven Press, 1990: 57-77
148. Insall J, Bullogh PG, Burstein AH. Proximal tube realignment
of the patella for chondromalacia patellae. Clin Orthop 1979;
144: 63-9
149. Scuderi G, Cuomo F, Scott WN. Lateral release and proximal
realignment for patellar subluxation and dislocation: a longterm follow-up. J Bone Joint Surg Am 1988; 70 (6): 856-61
150. Fielding JW, Liebler WA, Tambakis A. The effect of a tibial-tubercle transplant in children on the growth of the upper
tibial epiphysis. J Bone Joint Surg Am 1960; 42: 1426-34
151. Cox JS. Evaluation of the Roux-Elmslie-Trillat procedure for
knee extensor realignment. Am J Sports Med 1982; 10: 303-10
152. Ferguson Jr AB, Brown TD, Fu FH, et al. Relief of patellofemoral
contact stress by anterior displacement of the tibial tubercle.
J Bone Joint Surg Am 1979; 61 (2): 159-66
153. Maquet P. Mechanics and osteoarthritis of the patello-femoral
joint. Clin Orthop 1979; 144: 70-3
154. Engebretsen L, Svenningsen S, Benum P. Advancement of the
tibial tuberosity for patellar pain: a 5-year follow-up. Acta
Orthop Scand 1989; 60: 20-2
155. Radin EL, Pan HQ. Long term follow-up study on the Maquet
procedure with special reference to the causes of failure. Clin
Orthop 1993; 290: 253-8
156. Fulkerson JP. Anteromedialization of the tibial tuberosity for
patello-femoral malalignment. Clin Orthop 1983; 177: 176-81
157. Ficat RP, Ficat C, Gedeon P, et al. Spongialization: a new treatment for diseased patellae. Clin Orthop 1979; 144; 74-83
158. Papagelopoulos PJ, Sim FH. Patellofemoral pain syndrome: diagnosis and management. Orthopaedics 1997; 20: 148-57
Correspondence and reprints: Dr Roland Thome, Muscle Laboratory, Department of Rehabilitation Medicine, Sahlgrenska
University Hospital, Sahlgrenska, Guldhedsgatan 19, 41345
Gteborg, Sweden.
E-mail: roland.thomee@telia.com
Sports Med 1999 Oct; 28 (4)
Das könnte Ihnen auch gefallen
- Who Is Russ FinchDokument1 SeiteWho Is Russ FinchKtomislavNoch keine Bewertungen
- Why Is Scribd BadDokument1 SeiteWhy Is Scribd BadKtomislavNoch keine Bewertungen
- What Was The Recent Breakthrough in Fusion ResearchDokument1 SeiteWhat Was The Recent Breakthrough in Fusion ResearchKtomislavNoch keine Bewertungen
- Why Is Scribd GoodDokument1 SeiteWhy Is Scribd GoodKtomislavNoch keine Bewertungen
- Who Is Behind ScribdDokument1 SeiteWho Is Behind ScribdKtomislavNoch keine Bewertungen
- Gracie DietDokument57 SeitenGracie DietCamila Carioni de Ávila100% (4)
- Free Dont Wear Your Gi To The Bar ArtechokepdfDokument164 SeitenFree Dont Wear Your Gi To The Bar Artechokepdf1983gonzo100% (1)
- Risk Free BettingDokument20 SeitenRisk Free BettingKtomislav43% (7)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Trochanteric Bursitis Exercises Dec 5Dokument18 SeitenTrochanteric Bursitis Exercises Dec 5CoupleFF BRNoch keine Bewertungen
- ATHLETE HITT-Build Your Own WorkoutDokument10 SeitenATHLETE HITT-Build Your Own WorkoutAlfredo QuiñonesNoch keine Bewertungen
- Operative ArthrosDokument1.115 SeitenOperative ArthrosFabio Sales Vieira100% (6)
- Booty (Gym) : 50 Min LegsDokument6 SeitenBooty (Gym) : 50 Min LegsLucia Milagros Perea VillacrezNoch keine Bewertungen
- Hamstring Stretches: About This TopicDokument3 SeitenHamstring Stretches: About This Topicfurkann91Noch keine Bewertungen
- Nursing Lecture OrthopedicDokument24 SeitenNursing Lecture OrthopedicAedge010100% (2)
- ACL RSI Transcultural LCADokument8 SeitenACL RSI Transcultural LCAGuilhermeAndradeNoch keine Bewertungen
- AAOS Essentials of MusculoskeletalDokument1.295 SeitenAAOS Essentials of MusculoskeletalОлександр Шендера100% (6)
- Ultimate Performance Online ADVANCED ABSDokument2 SeitenUltimate Performance Online ADVANCED ABSSheiraj BatisteNoch keine Bewertungen
- The Ultimate Stretching ManualDokument193 SeitenThe Ultimate Stretching ManualAlessio AlfeiNoch keine Bewertungen
- Ortho Assessment PDFDokument9 SeitenOrtho Assessment PDFtafelaNoch keine Bewertungen
- ANAT1012.1019 Example Regional Lower Limb SAQ's - 2022Dokument3 SeitenANAT1012.1019 Example Regional Lower Limb SAQ's - 2022Grace YNoch keine Bewertungen
- Podcast en Ingles Keith BaarDokument14 SeitenPodcast en Ingles Keith BaarhectorNoch keine Bewertungen
- HFS Technique Manual PDFDokument39 SeitenHFS Technique Manual PDFbernard_heinrichNoch keine Bewertungen
- Transtibial AmputationDokument24 SeitenTranstibial Amputationokida192Noch keine Bewertungen
- Tuberculosis of KneeDokument17 SeitenTuberculosis of KneeJithin Bhagavati KalamNoch keine Bewertungen
- Preventing Musculoskeletal InjuryDokument18 SeitenPreventing Musculoskeletal InjuryPanida YaithummasarnNoch keine Bewertungen
- WorkoutsDokument13 SeitenWorkoutsMilena Thumbelina91% (11)
- Anatomy Lower Limb Sem. 1 - ProProfs QuizDokument26 SeitenAnatomy Lower Limb Sem. 1 - ProProfs QuizAhmedNoch keine Bewertungen
- Running Fitness - December 2015 PDFDokument100 SeitenRunning Fitness - December 2015 PDFknuprebycNoch keine Bewertungen
- Borut Fonda InpressDokument25 SeitenBorut Fonda InpressMarcelo CarvalhoNoch keine Bewertungen
- Prosthetics and Orthotics Manufacturing Guidelines: Lower Limb Prosthetics: Trans-Femoral ProsthesisDokument51 SeitenProsthetics and Orthotics Manufacturing Guidelines: Lower Limb Prosthetics: Trans-Femoral ProsthesisInternational Committee of the Red Cross50% (2)
- Functional Core StabilizationDokument71 SeitenFunctional Core StabilizationFábio De Ávila Peres100% (3)
- Hip Joint DislocationDokument59 SeitenHip Joint DislocationAnonymous P5FDn81yNoch keine Bewertungen
- ArthritisDokument406 SeitenArthritiskikria100% (2)
- AJO - Review of Common Clinical Conditions of The Proximal Tibiofibular Joint - 2018-12-12Dokument15 SeitenAJO - Review of Common Clinical Conditions of The Proximal Tibiofibular Joint - 2018-12-12pnalamati100% (1)
- ACL Technique GuideDokument8 SeitenACL Technique GuideDIMITRISNoch keine Bewertungen
- Stew Smith's 1.5 - 2 Mile Timed Run Training ProgramDokument15 SeitenStew Smith's 1.5 - 2 Mile Timed Run Training ProgramJohn RohrerNoch keine Bewertungen
- PASSORDokument38 SeitenPASSORDario TorresNoch keine Bewertungen
- Panf 2014 en PDFDokument124 SeitenPanf 2014 en PDFDavid BravoNoch keine Bewertungen