Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Four Front Music Marketing PlanDokument12 SeitenFour Front Music Marketing Planezrents100% (1)
- L O G B: The 5-Minute Personality TestDokument5 SeitenL O G B: The 5-Minute Personality TestezrentsNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Genesis 6 4 Did Angels Marry HumansDokument9 SeitenGenesis 6 4 Did Angels Marry Humansezrents0% (2)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- This Should Also Never Be Attempted IndoorsDokument11 SeitenThis Should Also Never Be Attempted IndoorsezrentsNoch keine Bewertungen
- RICS Damages For Delay To CompletionDokument20 SeitenRICS Damages For Delay To CompletionJon Smith100% (7)
- Is Someone A True Prophet of GodDokument91 SeitenIs Someone A True Prophet of GodezrentsNoch keine Bewertungen
- Clarion Printing House, Inc Vs NLRC Case DigestDokument2 SeitenClarion Printing House, Inc Vs NLRC Case Digestlaila ursabiaNoch keine Bewertungen
- Development Bank of The Philippines v. The Hon. Secretary of Labor, Cresencia Difontorum, Et AlDokument2 SeitenDevelopment Bank of The Philippines v. The Hon. Secretary of Labor, Cresencia Difontorum, Et AlKriselNoch keine Bewertungen
- Concept of Land Ownership in KenyaDokument14 SeitenConcept of Land Ownership in KenyaFrancis Njihia KaburuNoch keine Bewertungen
- Llorente v. Star City 05082020Dokument2 SeitenLlorente v. Star City 05082020Carlo Pajo0% (1)
- Referral Agreement (Referrals To Diamond Realty Brokers)Dokument1 SeiteReferral Agreement (Referrals To Diamond Realty Brokers)Angel KnightNoch keine Bewertungen
- 35 Country Bankers Insurance V CADokument2 Seiten35 Country Bankers Insurance V CAGabriel CruzNoch keine Bewertungen
- Orgasmic Fractionation 4 of 5Dokument1 SeiteOrgasmic Fractionation 4 of 5ezrentsNoch keine Bewertungen
- Orgasmic Fractionation 2 of 5Dokument1 SeiteOrgasmic Fractionation 2 of 5ezrentsNoch keine Bewertungen
- Our Part in The Sanctification ProcessDokument3 SeitenOur Part in The Sanctification ProcessezrentsNoch keine Bewertungen
- Orgasmic Fractionation 1 of 5Dokument1 SeiteOrgasmic Fractionation 1 of 5ezrentsNoch keine Bewertungen
- Orgasmic Fractionation 3 of 5Dokument1 SeiteOrgasmic Fractionation 3 of 5ezrentsNoch keine Bewertungen
- How To Build Operations Plan in 5 Easy StepsDokument3 SeitenHow To Build Operations Plan in 5 Easy StepsezrentsNoch keine Bewertungen
- Angels Servants of GodDokument6 SeitenAngels Servants of GodezrentsNoch keine Bewertungen
- Dreams EditDokument37 SeitenDreams EditezrentsNoch keine Bewertungen
- Systems of Equations Substitution PDFDokument4 SeitenSystems of Equations Substitution PDFezrentsNoch keine Bewertungen
- Linear Word ProblemsDokument7 SeitenLinear Word ProblemsnomnomNoch keine Bewertungen
- Four Front Music Marketing PlanDokument12 SeitenFour Front Music Marketing PlanezrentsNoch keine Bewertungen
- Baptism EditDokument7 SeitenBaptism EditezrentsNoch keine Bewertungen
- DOCS - 543506-V1-Power of Attorney Abdul Rahman AldawoodDokument3 SeitenDOCS - 543506-V1-Power of Attorney Abdul Rahman AldawoodDar AlfarooqNoch keine Bewertungen
- Business To Business PresentationDokument32 SeitenBusiness To Business PresentationezrentsNoch keine Bewertungen
- PROPERTY REVIEWER - Usufruct To EasementsDokument4 SeitenPROPERTY REVIEWER - Usufruct To EasementsChameNoch keine Bewertungen
- NegoDokument2 SeitenNegoVal Charles C. RingorNoch keine Bewertungen
- Confidential Non-Disclosure AgreementDokument1 SeiteConfidential Non-Disclosure AgreementTammie WalkerNoch keine Bewertungen
- Gemc 511687702766611 03022022Dokument8 SeitenGemc 511687702766611 03022022Awadh GroupNoch keine Bewertungen
- Citec International SN BHDDokument2 SeitenCitec International SN BHDAishath ShabaabNoch keine Bewertungen
- Palacios v. Ramirez Full TextDokument8 SeitenPalacios v. Ramirez Full TextJeng PionNoch keine Bewertungen
- VOL. 214, OCTOBER 7, 1992 475: Juarez vs. Court of AppealsDokument10 SeitenVOL. 214, OCTOBER 7, 1992 475: Juarez vs. Court of AppealsEver AlcazarNoch keine Bewertungen
- Information Technology, Broadcasting, Advertising, The Entertainment Industry, Censorship, and Internet and Online Services Among OthersDokument4 SeitenInformation Technology, Broadcasting, Advertising, The Entertainment Industry, Censorship, and Internet and Online Services Among OthersSharon AmondiNoch keine Bewertungen
- Directors & Officers Liability InsuranceDokument24 SeitenDirectors & Officers Liability InsuranceDivyanshu MishraNoch keine Bewertungen
- Instructor Manual For Financial & Managerial Accounting 16th (Sixteenth) Edition by Jan R. Williams, Sue F. Haka, Mark S. Bettner, Joseph V. CarcelloDokument7 SeitenInstructor Manual For Financial & Managerial Accounting 16th (Sixteenth) Edition by Jan R. Williams, Sue F. Haka, Mark S. Bettner, Joseph V. CarcelloJonathonChavezbcsj100% (15)
- Confidentiality Agreement Template Download 20171212Dokument3 SeitenConfidentiality Agreement Template Download 20171212Rahul AgnihotriNoch keine Bewertungen
- 4701 Ewing DR Castro Valley-Shivjoti PriharpDokument1 Seite4701 Ewing DR Castro Valley-Shivjoti PriharpLakshmi GaddeNoch keine Bewertungen
- Room Rental AgreementDokument4 SeitenRoom Rental AgreementJoebell VillanuevaNoch keine Bewertungen
- Topa NotesDokument74 SeitenTopa NotesSumerNoch keine Bewertungen
- Sneha Contract2 PDFDokument14 SeitenSneha Contract2 PDFSNEHA CANoch keine Bewertungen
- Deed of Usufructuary MortgageDokument1 SeiteDeed of Usufructuary MortgageNeelam Shujahuddin100% (1)
- Bus Pass FormDokument4 SeitenBus Pass Formshivchaudhary20954Noch keine Bewertungen
- Deed of Sale - Motor VehicleDokument4 SeitenDeed of Sale - Motor Vehiclekyle domingoNoch keine Bewertungen
- RBRDE740-TR01 Parts BookDokument123 SeitenRBRDE740-TR01 Parts BookCARLOS JOAQUIN CERNA VARGASNoch keine Bewertungen
- Financial Derivatives (Finance Specialization) (2019 Admission) 2022 MarchDokument6 SeitenFinancial Derivatives (Finance Specialization) (2019 Admission) 2022 MarchkcashiquaNoch keine Bewertungen
- Secured Transactions 2014Dokument4 SeitenSecured Transactions 2014Meng GoblasNoch keine Bewertungen
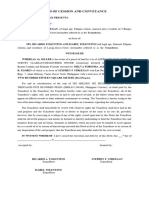
- DEED OF CESSION AND CONVEYANCE - LOT RICARDO TOLENTINO AND ISABELITA TOLENTINO 550kDokument2 SeitenDEED OF CESSION AND CONVEYANCE - LOT RICARDO TOLENTINO AND ISABELITA TOLENTINO 550klawrence.streegan5Noch keine Bewertungen