Das könnte Ihnen auch gefallen
- Project Management A Technicians Guide Staples TOCDokument5 SeitenProject Management A Technicians Guide Staples TOCAnonymous NwnJNO0% (3)
- Comparative Study of UK, USA and Indian Health Care SystemDokument12 SeitenComparative Study of UK, USA and Indian Health Care SystemArnab Chatterjee67% (3)
- Health ModelDokument41 SeitenHealth ModelMayom Mabuong100% (3)
- Appendix B - Distance Tables - Metric Units PDFDokument15 SeitenAppendix B - Distance Tables - Metric Units PDFitisINoch keine Bewertungen
- Austrilia Health CareDokument23 SeitenAustrilia Health CarePandaman PandaNoch keine Bewertungen
- Border Collie Training GuidelinesDokument12 SeitenBorder Collie Training GuidelinespsmanasseNoch keine Bewertungen
- AMS 48 - 2000-n - D0114354 - 055 - 00Dokument116 SeitenAMS 48 - 2000-n - D0114354 - 055 - 00wanhall100% (1)
- 6 Kuliah Liver CirrhosisDokument55 Seiten6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Intl Profiles FranceDokument5 SeitenIntl Profiles FranceJesse M. MassieNoch keine Bewertungen
- Presentation On Health Care System ModelsDokument37 SeitenPresentation On Health Care System ModelsTashi Makpen100% (1)
- Sik Weny LoboDokument15 SeitenSik Weny LobonoviNoch keine Bewertungen
- Health Care SystemDokument5 SeitenHealth Care SystemadelekeyusufNoch keine Bewertungen
- Hospital Building Assignments 2Dokument34 SeitenHospital Building Assignments 2sintu kumarNoch keine Bewertungen
- Healthcare System in RomaniaDokument14 SeitenHealthcare System in RomaniaanitudoseNoch keine Bewertungen
- Healthcare System of AustraliaDokument12 SeitenHealthcare System of Australiakhan1818Noch keine Bewertungen
- The Italian Healthcare SystemDokument5 SeitenThe Italian Healthcare SystemAnnamaria FrezzaNoch keine Bewertungen
- Comparative Healthcare SystemsDokument95 SeitenComparative Healthcare SystemsLuiggi GordilloNoch keine Bewertungen
- His Lab Prelim NotesDokument14 SeitenHis Lab Prelim NotesJuren LasagaNoch keine Bewertungen
- Health System Model of VietnamDokument20 SeitenHealth System Model of Vietnamsneha khuranaNoch keine Bewertungen
- Bulgaria PHIS Pharma ProfileDokument99 SeitenBulgaria PHIS Pharma ProfileportosinNoch keine Bewertungen
- Romania: Health Sector Policy Note I. Background and AccomplishmentsDokument11 SeitenRomania: Health Sector Policy Note I. Background and AccomplishmentsMaria Gabriela PopaNoch keine Bewertungen
- Philippine Health Insurance CorporationDokument7 SeitenPhilippine Health Insurance CorporationEllen Glae DaquipilNoch keine Bewertungen
- UK Country Profile 2008Dokument3 SeitenUK Country Profile 2008albajcNoch keine Bewertungen
- France Healthcare SystemsDokument20 SeitenFrance Healthcare SystemsRutvik GandhiNoch keine Bewertungen
- Healthcare System in AustraliaDokument19 SeitenHealthcare System in AustraliaVera YusufNoch keine Bewertungen
- Lecture 13-The Medical IndustryDokument4 SeitenLecture 13-The Medical IndustryMoses EagleNoch keine Bewertungen
- Medical Health Insurance Systems in Europe, USA, Canada, and AustraliaDokument13 SeitenMedical Health Insurance Systems in Europe, USA, Canada, and Australiaeko abiNoch keine Bewertungen
- 02chapter02 PDFDokument7 Seiten02chapter02 PDFAnonymous geItmk3Noch keine Bewertungen
- Understanding The NhiDokument8 SeitenUnderstanding The NhieNCA.comNoch keine Bewertungen
- The Indian Health Care SystemDokument9 SeitenThe Indian Health Care SystemAaron Michelle DuvaliNoch keine Bewertungen
- Service Delivery Profile VietnamDokument11 SeitenService Delivery Profile VietnamtkielczNoch keine Bewertungen
- Health Care System of The Philippines and Switzerland PhilippinesDokument2 SeitenHealth Care System of The Philippines and Switzerland PhilippinesJohn Adrian MaulionNoch keine Bewertungen
- Health Care Lessons From DenmarkDokument6 SeitenHealth Care Lessons From DenmarkCarol LaytonNoch keine Bewertungen
- India Health PrimerDokument35 SeitenIndia Health PrimerPoorny PurushothNoch keine Bewertungen
- Health Care Schemes Project at KamineniDokument78 SeitenHealth Care Schemes Project at KamineniVenugopal VutukuruNoch keine Bewertungen
- In The Name of Allah, The Most Beneficent, The Most Gracious, The Most Merciful!Dokument12 SeitenIn The Name of Allah, The Most Beneficent, The Most Gracious, The Most Merciful!sana181019811Noch keine Bewertungen
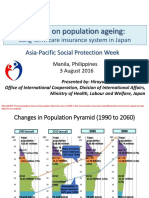
- APSP - Session 9A - Hiroyuki Yamaya - MHLWDokument8 SeitenAPSP - Session 9A - Hiroyuki Yamaya - MHLWKristine PresbiteroNoch keine Bewertungen
- One Your ShillDokument4 SeitenOne Your ShillSupron AlimudinNoch keine Bewertungen
- Health System in IndiaDokument36 SeitenHealth System in IndiaRishi RanjanNoch keine Bewertungen
- Healthcare System in JapanDokument4 SeitenHealthcare System in JapanBayuAkbarSyarifNoch keine Bewertungen
- Norway: - EU Manual of Dental Practice: Version 4 (2008)Dokument10 SeitenNorway: - EU Manual of Dental Practice: Version 4 (2008)ahmed_awad_36Noch keine Bewertungen
- Cea Private Medical InsuranceDokument20 SeitenCea Private Medical Insurancemaslinovik5003Noch keine Bewertungen
- RC2 - TxtEnglishHealthcareSystemDokument2 SeitenRC2 - TxtEnglishHealthcareSystemMaximeNoch keine Bewertungen
- Healthcare SystemsDokument2 SeitenHealthcare SystemsFlor IgartuaNoch keine Bewertungen
- Reviewer Philhealth 2Dokument7 SeitenReviewer Philhealth 2Lerma EstoboNoch keine Bewertungen
- UHCPresentations 2 2010oct (Annex 17) AAPadillaDokument38 SeitenUHCPresentations 2 2010oct (Annex 17) AAPadillaKarl Marxcuz ReyesNoch keine Bewertungen
- Health Inequities by Rama Baru PDFDokument6 SeitenHealth Inequities by Rama Baru PDFwrit majumdarNoch keine Bewertungen
- Nu710 w5 - Paper International Healthcare SystemsDokument11 SeitenNu710 w5 - Paper International Healthcare Systemsapi-577441503Noch keine Bewertungen
- Health System in India: Tej Ram JatDokument20 SeitenHealth System in India: Tej Ram JatAmit Risky VermaNoch keine Bewertungen
- Health Care SystemDokument43 SeitenHealth Care SystemAlexa Abidin Oldenborg100% (1)
- Healthcare in GermanyDokument6 SeitenHealthcare in GermanyAkash ShahNoch keine Bewertungen
- En WP Money in MedicineDokument26 SeitenEn WP Money in MedicineJehad Al yousefNoch keine Bewertungen
- Sistem ImunDokument16 SeitenSistem ImunDwii N AriiyantooNoch keine Bewertungen
- Global Typologies of Healthcare SystemsDokument12 SeitenGlobal Typologies of Healthcare SystemstewodrosbayisaNoch keine Bewertungen
- Healthcare 200729042655Dokument22 SeitenHealthcare 200729042655Khalid Md BahauddinNoch keine Bewertungen
- Comparative Models of Healthcare System: Canada: Group 6ADokument13 SeitenComparative Models of Healthcare System: Canada: Group 6AAnonymouscat100% (1)
- MekdishaaaaaDokument12 SeitenMekdishaaaaatewodros bayisaNoch keine Bewertungen
- Swedish Health Care SystemDokument2 SeitenSwedish Health Care SystemHassaan KarimNoch keine Bewertungen
- Healthcare in IndiaDokument40 SeitenHealthcare in Indiamanisha paikaray100% (1)
- Spain Healthcare SystemDokument5 SeitenSpain Healthcare SystemAbhinav NarayanNoch keine Bewertungen
- Health Care Models: International Comparisons: Dr. Jaime Llambías-Wolff, Ph.D. York UniversityDokument22 SeitenHealth Care Models: International Comparisons: Dr. Jaime Llambías-Wolff, Ph.D. York UniversityTas SafetyTradeNoch keine Bewertungen
- medical english作業 PDFDokument10 Seitenmedical english作業 PDFeric483460Noch keine Bewertungen
- Health Practices of CanadaDokument17 SeitenHealth Practices of CanadasnehaoctNoch keine Bewertungen
- Achieving the Human Right to a Caring Society in an Aging AmericaVon EverandAchieving the Human Right to a Caring Society in an Aging AmericaNoch keine Bewertungen
- SahDokument4 SeitenSahNofalyaKamalinNoch keine Bewertungen
- Narative HunchbackDokument2 SeitenNarative HunchbackNofalyaKamalinNoch keine Bewertungen
- Primary Infection With Varicella-Zoster VirusDokument8 SeitenPrimary Infection With Varicella-Zoster VirusNofalyaKamalinNoch keine Bewertungen
- Indonesia Health System - ArticleDokument7 SeitenIndonesia Health System - ArticleNofalyaKamalinNoch keine Bewertungen
- Sp. Observed Every 12 Hours Starting From The Larval Stage of Flies From OneDokument1 SeiteSp. Observed Every 12 Hours Starting From The Larval Stage of Flies From OneNofalyaKamalinNoch keine Bewertungen
- PMI IDI Ikatan Dokter Indonesia ... 12 ATP Tess Aapcc Spss 29Dokument1 SeitePMI IDI Ikatan Dokter Indonesia ... 12 ATP Tess Aapcc Spss 29NofalyaKamalinNoch keine Bewertungen
- Daily Staff Food Consumption Reports Sep-2019Dokument4 SeitenDaily Staff Food Consumption Reports Sep-2019Manjit RawatNoch keine Bewertungen
- Unit 8 Packet KeyDokument21 SeitenUnit 8 Packet KeyHiddenNoch keine Bewertungen
- Epicor Software India Private Limited: Brief Details of Your Form-16 Are As UnderDokument9 SeitenEpicor Software India Private Limited: Brief Details of Your Form-16 Are As UndersudhadkNoch keine Bewertungen
- Transfer and Business Taxation SyllabusDokument5 SeitenTransfer and Business Taxation SyllabusamqqndeahdgeNoch keine Bewertungen
- ALL102-Walker Shirley-Unemployed at Last-The Monkeys Mask and The Poetics of Excision-Pp72-85Dokument15 SeitenALL102-Walker Shirley-Unemployed at Last-The Monkeys Mask and The Poetics of Excision-Pp72-85PNoch keine Bewertungen
- Drug-Nutrient Interaction in Prescriptions ForDokument7 SeitenDrug-Nutrient Interaction in Prescriptions ForRafika DitaNoch keine Bewertungen
- ISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixDokument3 SeitenISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixvenkatesanNoch keine Bewertungen
- Far Eastern University - Manila Income Taxation TAX1101 Fringe Benefit TaxDokument10 SeitenFar Eastern University - Manila Income Taxation TAX1101 Fringe Benefit TaxRyan Christian BalanquitNoch keine Bewertungen
- Home Composting SystemsDokument8 SeitenHome Composting Systemssumanenthiran123Noch keine Bewertungen
- Mainstreaming Gad Budget in The SDPDokument14 SeitenMainstreaming Gad Budget in The SDPprecillaugartehalagoNoch keine Bewertungen
- Dressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionDokument2 SeitenDressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionAlvaCatalinaNoch keine Bewertungen
- OPSS1213 Mar98Dokument3 SeitenOPSS1213 Mar98Tony ParkNoch keine Bewertungen
- Riber 6-s1 SP s17-097 336-344Dokument9 SeitenRiber 6-s1 SP s17-097 336-344ᎷᏒ'ᏴᎬᎪᏚᎢ ᎷᏒ'ᏴᎬᎪᏚᎢNoch keine Bewertungen
- Employment Offer: 1. Employer InformationDokument2 SeitenEmployment Offer: 1. Employer InformationnavidNoch keine Bewertungen
- Conference Version of SB 1Dokument486 SeitenConference Version of SB 1Paul MastersNoch keine Bewertungen
- Outlook 2Dokument188 SeitenOutlook 2Mafer Garces NeuhausNoch keine Bewertungen
- Tamilnadu Shop and Establishment ActDokument6 SeitenTamilnadu Shop and Establishment ActShiny VargheesNoch keine Bewertungen
- Brief RESUME EmailDokument4 SeitenBrief RESUME Emailranjit_kadalg2011Noch keine Bewertungen
- DT 2107Dokument1 SeiteDT 2107Richard PeriyanayagamNoch keine Bewertungen
- QA-QC TPL of Ecube LabDokument1 SeiteQA-QC TPL of Ecube LabManash Protim GogoiNoch keine Bewertungen
- Oil ShaleDokument13 SeitenOil Shalergopi_83Noch keine Bewertungen
- Demages Goods RecordDokument22 SeitenDemages Goods Recordtariq malikNoch keine Bewertungen
- Lesson 1 - Intro To Highway EngineeringDokument15 SeitenLesson 1 - Intro To Highway EngineeringSaoirseNoch keine Bewertungen
- E61 DiagramDokument79 SeitenE61 Diagramthanes1027Noch keine Bewertungen
- Penilaian Akhir TahunDokument4 SeitenPenilaian Akhir TahunRestu Suci UtamiNoch keine Bewertungen