Das könnte Ihnen auch gefallen
- Piaggio X8 250 I.E. (EN)Dokument289 SeitenPiaggio X8 250 I.E. (EN)Manualles100% (8)
- Data Center Report TemplateDokument17 SeitenData Center Report TemplateHussien Mobark100% (3)
- D20 ECDIS - Gyro Input FailureDokument1 SeiteD20 ECDIS - Gyro Input FailureRiaz Ahmed67% (3)
- BOOST ExamplesDokument128 SeitenBOOST Examplesiturcic9Noch keine Bewertungen
- D18 ECDIS - Speed Log Input FailureDokument1 SeiteD18 ECDIS - Speed Log Input FailureRiaz AhmedNoch keine Bewertungen
- D17 ECDIS - GPS Input FailureDokument1 SeiteD17 ECDIS - GPS Input FailureRiaz Ahmed100% (1)
- SAF16 - Critical Operations Checklist: Ships Name: Department Checklist NoDokument1 SeiteSAF16 - Critical Operations Checklist: Ships Name: Department Checklist NoRiaz AhmedNoch keine Bewertungen
- Shackle Marking InformationDokument7 SeitenShackle Marking Informationmalborn100% (1)
- New Model For Predicting Thermal Radiation From Flares and High Pressure Jet Fires For Hydrogen and SyngasDokument15 SeitenNew Model For Predicting Thermal Radiation From Flares and High Pressure Jet Fires For Hydrogen and Syngasthlim19078656Noch keine Bewertungen
- 2322 Weekly CheckDokument2 Seiten2322 Weekly CheckR ShindeNoch keine Bewertungen
- U. S. Army Corps of Engineers Above-Ground Treatment System Performance ChecklistDokument8 SeitenU. S. Army Corps of Engineers Above-Ground Treatment System Performance Checklistavisek_basuNoch keine Bewertungen
- Pre-Review Facility EH&S Questionnaire: I. Site Description, Vicinity, and HistoryDokument17 SeitenPre-Review Facility EH&S Questionnaire: I. Site Description, Vicinity, and HistoryDemilade FasinaNoch keine Bewertungen
- Dredge Fox River Operators Daily ReportDokument15 SeitenDredge Fox River Operators Daily ReportPhilip NguyenNoch keine Bewertungen
- TM 11 6625 316 12Dokument83 SeitenTM 11 6625 316 12Costas MoraitisNoch keine Bewertungen
- Eohsms-02-C18 Loa WSH CoordinatorDokument2 SeitenEohsms-02-C18 Loa WSH CoordinatorHassan AbdullahNoch keine Bewertungen
- Q-Exactive-GC Preinstallation GuideDokument67 SeitenQ-Exactive-GC Preinstallation GuideDiego BermudezNoch keine Bewertungen
- DENR-EMB QSMR 1st Quarter Jan-Mar2020Dokument8 SeitenDENR-EMB QSMR 1st Quarter Jan-Mar2020Jennifer DYNoch keine Bewertungen
- Engine Room DocumentsDokument5 SeitenEngine Room DocumentsФурад ДжакумовNoch keine Bewertungen
- Form C-6: Inspection ChecklistDokument4 SeitenForm C-6: Inspection ChecklistAj Carmona IINoch keine Bewertungen
- SoilVaporExtraction SubsurfaceDokument8 SeitenSoilVaporExtraction SubsurfaceAugusto PetryNoch keine Bewertungen
- Fitri Arshad - 2.4Dokument1 SeiteFitri Arshad - 2.4Fitrie ArshadzNoch keine Bewertungen
- USCG Abandon N Fire DrillDokument5 SeitenUSCG Abandon N Fire DrillAdrian CretuNoch keine Bewertungen
- CW FUSION PM Checklist - M-QF-75-11 Rev ADokument2 SeitenCW FUSION PM Checklist - M-QF-75-11 Rev AbaileybancroftNoch keine Bewertungen
- ESI Oil Sampling SheetDokument1 SeiteESI Oil Sampling SheetGM PNoch keine Bewertungen
- Inter TankoDokument2 SeitenInter Tankoch3g44100% (1)
- Annual Sprinkler Inspection FormDokument4 SeitenAnnual Sprinkler Inspection FormBryan NavarroNoch keine Bewertungen
- Barford TR5048 Manual + Parts List 2021 WITH MULCHDokument62 SeitenBarford TR5048 Manual + Parts List 2021 WITH MULCHpggmarquesNoch keine Bewertungen
- Environment Audit Report Format - GPCBDokument8 SeitenEnvironment Audit Report Format - GPCBmaikalrNoch keine Bewertungen
- Engineering and Operations LOTO Annual InspectionDokument3 SeitenEngineering and Operations LOTO Annual InspectionEslam IsmailNoch keine Bewertungen
- Engine Repair ILT Participant GuideDokument15 SeitenEngine Repair ILT Participant Guidejordan navarroNoch keine Bewertungen
- Manual 1Dokument59 SeitenManual 1Walter DelgadoNoch keine Bewertungen
- Standard Field Report Standard Specification - MCE EG020 CDokument11 SeitenStandard Field Report Standard Specification - MCE EG020 CSenol LimanNoch keine Bewertungen
- SPT Boat SurveyDokument2 SeitenSPT Boat Surveyjgrav667Noch keine Bewertungen
- Blank Well Log PDFDokument3 SeitenBlank Well Log PDFJordi EscorciaNoch keine Bewertungen
- Reference Tank Handbook PDFDokument10 SeitenReference Tank Handbook PDFIvan AvilesNoch keine Bewertungen
- Checklist To Master Dry Dock Operations - Deck Department (Vessel General Dry Dock Hull Work Report)Dokument1 SeiteChecklist To Master Dry Dock Operations - Deck Department (Vessel General Dry Dock Hull Work Report)George MihalceaNoch keine Bewertungen
- ER-10-4-01 EN Installation List Data and Start Up ChecksDokument9 SeitenER-10-4-01 EN Installation List Data and Start Up ChecksCamilo Andres Cardozo FajardoNoch keine Bewertungen
- Er 10 4 01Dokument8 SeitenEr 10 4 01Mohammad Shafaet JamilNoch keine Bewertungen
- FM 03 501Dokument68 SeitenFM 03 501Wika SentiongNoch keine Bewertungen
- F-030-Diesel Generator Inspection ChecklistDokument1 SeiteF-030-Diesel Generator Inspection ChecklistAbdus SamadNoch keine Bewertungen
- F-030-Diesel Generator Inspection ChecklistDokument1 SeiteF-030-Diesel Generator Inspection ChecklistDedy Rifky SetyawanNoch keine Bewertungen
- ProFloSe UF UseDokument2 SeitenProFloSe UF UseintermountainwaterNoch keine Bewertungen
- Asme U1 FormsDokument4 SeitenAsme U1 FormsoberaiNoch keine Bewertungen
- Leak Detection and RepairDokument8 SeitenLeak Detection and RepairNos GoteNoch keine Bewertungen
- NSRP Testing ProcedureDokument502 SeitenNSRP Testing Procedurecharlie limNoch keine Bewertungen
- ELFL004Dokument15 SeitenELFL004Destry YoungNoch keine Bewertungen
- Ops Plan TempDokument24 SeitenOps Plan TempR ShindeNoch keine Bewertungen
- Aramco Ticket No.: Eqpm'T Number: Service Date: Service LocationDokument4 SeitenAramco Ticket No.: Eqpm'T Number: Service Date: Service LocationArt AlbastroNoch keine Bewertungen
- Water SamplingDokument5 SeitenWater SamplingroldskiNoch keine Bewertungen
- MSC.1-Circ.980-Add.1 - (Continued) (Secretariat)Dokument218 SeitenMSC.1-Circ.980-Add.1 - (Continued) (Secretariat)K.l. DhanaNoch keine Bewertungen
- SupplierQuestionnaire SectionA General Info ModifiedDokument12 SeitenSupplierQuestionnaire SectionA General Info ModifieddsevolveNoch keine Bewertungen
- 21 50 51Dokument100 Seiten21 50 51flitecomponentsNoch keine Bewertungen
- SP2000 COD Testkits 2014Dokument5 SeitenSP2000 COD Testkits 2014Andres FalmacelNoch keine Bewertungen
- WPS 1013-2011Dokument27 SeitenWPS 1013-2011alexander100% (1)
- Jumping Compactor Inspection ChecklistDokument1 SeiteJumping Compactor Inspection Checklistarunjith rNoch keine Bewertungen
- Unit Gas Leak ChecklistDokument1 SeiteUnit Gas Leak Checklistfathul syaafNoch keine Bewertungen
- Flowmeter Preventive Maintenance FormDokument1 SeiteFlowmeter Preventive Maintenance FormWaseem TariqNoch keine Bewertungen
- You Will Be Able ToDokument104 SeitenYou Will Be Able ToSenorBublikNoch keine Bewertungen
- Ms. Norbelene B. Siat Nestfarms, Inc.: Ion XiDokument4 SeitenMs. Norbelene B. Siat Nestfarms, Inc.: Ion XiMelvinDapitanonNoch keine Bewertungen
- Warranty Notification - Installation List Data and Start Up Check Lists For Reciprocating Compressors JG:A:M:N:P:Q:R:J:H:E:K:T:C:D:FDokument9 SeitenWarranty Notification - Installation List Data and Start Up Check Lists For Reciprocating Compressors JG:A:M:N:P:Q:R:J:H:E:K:T:C:D:FMandava Subrahmanya Sivarama PrasadNoch keine Bewertungen
- TPI 2032120-2 - Loud Combustion Noises or Juddering at Light Acceleration, Engine Starts With DelayDokument5 SeitenTPI 2032120-2 - Loud Combustion Noises or Juddering at Light Acceleration, Engine Starts With DelayDavianGiurcaNoch keine Bewertungen
- DeclarationDokument1 SeiteDeclarationsmartfox1Noch keine Bewertungen
- Baldwin Field Report FormDokument2 SeitenBaldwin Field Report FormSMcNoch keine Bewertungen
- FRM SMRDokument8 SeitenFRM SMRAnonymous 8HnV4CAo100% (1)
- Annual Survey ChecklistDokument15 SeitenAnnual Survey ChecklistharryNoch keine Bewertungen
- Automotive Actuators and EVAP System TestingVon EverandAutomotive Actuators and EVAP System TestingBewertung: 4.5 von 5 Sternen4.5/5 (4)
- IMPORT (Load) : Sub - Total Workable VSSLDokument1 SeiteIMPORT (Load) : Sub - Total Workable VSSLRiaz AhmedNoch keine Bewertungen
- Korea Shipowners' AssociationDokument6 SeitenKorea Shipowners' AssociationRiaz AhmedNoch keine Bewertungen
- SGSClinker OmanDokument1 SeiteSGSClinker OmanRiaz AhmedNoch keine Bewertungen
- Ship BreakingDokument99 SeitenShip BreakingRiaz Ahmed100% (1)
- At A Glance Ship Berthing Data For CPADokument1 SeiteAt A Glance Ship Berthing Data For CPARiaz AhmedNoch keine Bewertungen
- VGP01 Routine Visual InspectionDokument3 SeitenVGP01 Routine Visual InspectionRiaz AhmedNoch keine Bewertungen
- Of Vessels: Dated: Berthing Position & PerformanceDokument2 SeitenOf Vessels: Dated: Berthing Position & PerformanceRiaz AhmedNoch keine Bewertungen
- VGP Final Permit2013Dokument194 SeitenVGP Final Permit2013Riaz AhmedNoch keine Bewertungen
- Frequently Asked Questions Update 20 Feb 2009Dokument1 SeiteFrequently Asked Questions Update 20 Feb 2009Riaz AhmedNoch keine Bewertungen
- VGP Faq 1Dokument3 SeitenVGP Faq 1Riaz AhmedNoch keine Bewertungen
- VGP Final Permit2013Dokument194 SeitenVGP Final Permit2013Riaz AhmedNoch keine Bewertungen
- VGP Logbook - Sample EntriesDokument13 SeitenVGP Logbook - Sample EntriesRiaz AhmedNoch keine Bewertungen
- Ecdis - Primary Ecdis FailureDokument1 SeiteEcdis - Primary Ecdis FailureRiaz AhmedNoch keine Bewertungen
- ECDIS - Failure of Secondary Means of NavigationDokument1 SeiteECDIS - Failure of Secondary Means of NavigationRiaz AhmedNoch keine Bewertungen
- (Ibn Al-Jawzi) Devils Deception (Talbis Iblis)Dokument70 Seiten(Ibn Al-Jawzi) Devils Deception (Talbis Iblis)shkmdNoch keine Bewertungen
- Midterm BUS510Dokument8 SeitenMidterm BUS510Ramesh KomarapuriNoch keine Bewertungen
- E Rich Burn Control System: With Stablesense™ TechnologyDokument4 SeitenE Rich Burn Control System: With Stablesense™ TechnologyYasir JamilNoch keine Bewertungen
- Mitchell-Banki Turbine Design Document PDFDokument37 SeitenMitchell-Banki Turbine Design Document PDFprojetosschillingNoch keine Bewertungen
- Chapter 2 Maternal Anatomy WilliamsDokument60 SeitenChapter 2 Maternal Anatomy WilliamsDiskaAstariniNoch keine Bewertungen
- P103154 - 7.00 - Doc - Manual - 8000 WindlassDokument43 SeitenP103154 - 7.00 - Doc - Manual - 8000 WindlassDanNoch keine Bewertungen
- Final Formula SheetDokument1 SeiteFinal Formula SheetFaryalNoch keine Bewertungen
- Chapter 1 - Steam GenerationDokument23 SeitenChapter 1 - Steam GenerationAzhan FikriNoch keine Bewertungen
- Part 1Dokument120 SeitenPart 1Raju Halder0% (1)
- Cortec, VpCI-371 Application GuideDokument2 SeitenCortec, VpCI-371 Application Guidemonserrat PereaNoch keine Bewertungen
- 8051 Serial CommunicationDokument35 Seiten8051 Serial CommunicationSanthosh CricketNoch keine Bewertungen
- AMC2019 StudentsResults Indonesia 8JDokument4 SeitenAMC2019 StudentsResults Indonesia 8JWinety Kristiana DewiNoch keine Bewertungen
- Processing Sequence When Posting An EventDokument5 SeitenProcessing Sequence When Posting An EventSrinivas ManchiNoch keine Bewertungen
- The Mathematical Society of Serbia - 60 YearsDokument23 SeitenThe Mathematical Society of Serbia - 60 YearsBranko Ma Branko TadicNoch keine Bewertungen
- Tarea Stereonet-HelpDokument32 SeitenTarea Stereonet-HelpJosueHuillcaPortilloNoch keine Bewertungen
- MTU-JB RadiatorsDokument11 SeitenMTU-JB Radiatorsnanthu7090Noch keine Bewertungen
- Sheet Pile Analysis Sheet v1.07-18.1Dokument2 SeitenSheet Pile Analysis Sheet v1.07-18.1SES DESIGN100% (1)
- Lecture 4: Expert Systems: What Is An Expert System?Dokument5 SeitenLecture 4: Expert Systems: What Is An Expert System?Zerihun BekeleNoch keine Bewertungen
- Maths Shortcuts by DayTodayGKDokument20 SeitenMaths Shortcuts by DayTodayGKAnand KesarkarNoch keine Bewertungen
- Pediatric Appendicitis ScoreDokument6 SeitenPediatric Appendicitis ScorePinandhito LatukolanNoch keine Bewertungen
- Manual Dimmer BukeDokument10 SeitenManual Dimmer BukeJavi KatzNoch keine Bewertungen
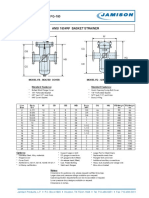
- FB-150 FQ-150 Basket StrainerDokument1 SeiteFB-150 FQ-150 Basket Strainerklich77Noch keine Bewertungen
- Caliper Xy MemoryDokument6 SeitenCaliper Xy MemoryA MuNoch keine Bewertungen
- Fire InvestigationDokument126 SeitenFire InvestigationAbcede IloiloNoch keine Bewertungen
- Midterm rp - Nguyễn Phú Minh Nhật - 20202795Dokument1 SeiteMidterm rp - Nguyễn Phú Minh Nhật - 20202795Minh Nhật100% (1)
- MMW (Data Management) - Part 2Dokument43 SeitenMMW (Data Management) - Part 2arabellah shainnah rosalesNoch keine Bewertungen
- DPP 01 Periodic Table JH Sir-3576 PDFDokument5 SeitenDPP 01 Periodic Table JH Sir-3576 PDFChessNoch keine Bewertungen
- MAJOR14Dokument14 SeitenMAJOR14swathi100% (1)