Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Regulatory Issues For Herbal Products - A ReviewDokument12 SeitenRegulatory Issues For Herbal Products - A Reviewvishal sachan100% (1)
- Furuncle AbsessDokument5 SeitenFuruncle AbsessDyah Nuriisa ANoch keine Bewertungen
- DubowitzDokument4 SeitenDubowitzDyah Nuriisa ANoch keine Bewertungen
- Multple MyelomaDokument11 SeitenMultple MyelomaDyah Nuriisa ANoch keine Bewertungen
- Ovarian Cyst AcogDokument2 SeitenOvarian Cyst AcogDyah Nuriisa ANoch keine Bewertungen
- Case ReflexionDokument2 SeitenCase ReflexionDyah Nuriisa ANoch keine Bewertungen
- Thuja PDFDokument3 SeitenThuja PDFDyah Nuriisa ANoch keine Bewertungen
- Neuropati Diabetes Dr. Audhy Tanasal SPSDokument41 SeitenNeuropati Diabetes Dr. Audhy Tanasal SPSNdel LindaNoch keine Bewertungen
- Status Epileptikus Non KonvulsifDokument10 SeitenStatus Epileptikus Non KonvulsifAhmad Riva'iNoch keine Bewertungen
- Chest PainDokument10 SeitenChest PainDyah Nuriisa ANoch keine Bewertungen
- Approach To The Adult Patient With Fever of Unknown OriginDokument6 SeitenApproach To The Adult Patient With Fever of Unknown Origini can always make u smile :D100% (1)
- AAFP - Evaluation of Acute Abdomen in AdultsDokument8 SeitenAAFP - Evaluation of Acute Abdomen in AdultsTe HineahuoneNoch keine Bewertungen
- Guideline Multiple MielomaDokument99 SeitenGuideline Multiple MielomamashitayuswiniNoch keine Bewertungen
- Cognitive Behavioral Theraphy For InsomniaDokument9 SeitenCognitive Behavioral Theraphy For InsomniaDyah Nuriisa ANoch keine Bewertungen
- Insecticides,: Plant and Animal PoisoningDokument56 SeitenInsecticides,: Plant and Animal PoisoningKrisna MuhammadNoch keine Bewertungen
- Laporan BiokimiaDokument2 SeitenLaporan BiokimiaDyah Nuriisa ANoch keine Bewertungen
- Dizziness: Classification and PathophysiologyDokument16 SeitenDizziness: Classification and Pathophysiologyrapannika100% (2)
- Maurice Nicoll The Mark PDFDokument4 SeitenMaurice Nicoll The Mark PDFErwin KroonNoch keine Bewertungen
- Cover Biokim CarotenDokument1 SeiteCover Biokim CarotenDyah Nuriisa ANoch keine Bewertungen
- All Other NZ McqsDokument36 SeitenAll Other NZ McqsTran Thai SonNoch keine Bewertungen
- Bioequivalence of 250 MG Lysine ClonixinDokument6 SeitenBioequivalence of 250 MG Lysine ClonixinMax Marcial JavierNoch keine Bewertungen
- NAME OF DRUG NozinanDokument3 SeitenNAME OF DRUG NozinanMill Jan CruzNoch keine Bewertungen
- Emulsions in Health Care Applications-An Overview: Journal of Dispersion Science and Technology May 2002Dokument24 SeitenEmulsions in Health Care Applications-An Overview: Journal of Dispersion Science and Technology May 2002Quốc ThắngNoch keine Bewertungen
- Pitocin: (Oxytocin Injection, USP) Synthetic DescriptionDokument7 SeitenPitocin: (Oxytocin Injection, USP) Synthetic Descriptionrevathidadam55555Noch keine Bewertungen
- Cluster HeadacheDokument14 SeitenCluster HeadacheadriantiariNoch keine Bewertungen
- Experiment 4 FWRDokument5 SeitenExperiment 4 FWRSarah HermosuraNoch keine Bewertungen
- 1st Quiz PharDokument4 Seiten1st Quiz PharnikhilNoch keine Bewertungen
- MethimazoleDokument5 SeitenMethimazoleapi-300595323Noch keine Bewertungen
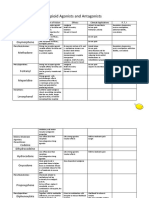
- Opioid Agonists and AntagonistsDokument5 SeitenOpioid Agonists and AntagonistsCas BuNoch keine Bewertungen
- Covovax ToDokument1 SeiteCovovax ToPrajasaktiNoch keine Bewertungen
- National Drug Policy/Generics Law: Romeo R. Andaya, MD, MSCPD, PHD, Fpafp Chair, DPMCH Uph-DjgtmuDokument14 SeitenNational Drug Policy/Generics Law: Romeo R. Andaya, MD, MSCPD, PHD, Fpafp Chair, DPMCH Uph-DjgtmuKatNoch keine Bewertungen
- Amr Thesis MergedDokument119 SeitenAmr Thesis Mergedm9966822Noch keine Bewertungen
- 2 CLINICAL PHARMACOLOGY - Prescription - WritingDokument52 Seiten2 CLINICAL PHARMACOLOGY - Prescription - Writingtf.almutairi88Noch keine Bewertungen
- Dose CalculationsDokument39 SeitenDose CalculationsAsma BakheitNoch keine Bewertungen
- Drug of Choice and DiseasesDokument2 SeitenDrug of Choice and DiseasesJamesNoch keine Bewertungen
- Drug Approval ProcessDokument514 SeitenDrug Approval ProcessMohan Varma0% (1)
- Pharmaceutical Industry: Powerpoint Templates Powerpoint TemplatesDokument22 SeitenPharmaceutical Industry: Powerpoint Templates Powerpoint TemplatesM Yasir AliNoch keine Bewertungen
- Adrif Vision List New 11.02.2021Dokument2 SeitenAdrif Vision List New 11.02.2021rahsreeNoch keine Bewertungen
- Charts For PharmacologyDokument3 SeitenCharts For PharmacologyAditi100% (1)
- D Jothiewari Et. Al.. (UV)Dokument5 SeitenD Jothiewari Et. Al.. (UV)EVELYN SOLANHS ACERO RODRIGUEZNoch keine Bewertungen
- SJC UzpharmsanoatDokument12 SeitenSJC UzpharmsanoatLVKonfederacijaNoch keine Bewertungen
- Clinically Preferred FormularyDokument42 SeitenClinically Preferred FormularyrajendickNoch keine Bewertungen
- Caroline M. Apovian - Body Weight Considerations in The Management of Type 2 DiabetesDokument15 SeitenCaroline M. Apovian - Body Weight Considerations in The Management of Type 2 DiabetesFarid RakhmanNoch keine Bewertungen
- Jchaput 2017 PHRMSCI177 Syll FVDokument4 SeitenJchaput 2017 PHRMSCI177 Syll FVVivian PhamNoch keine Bewertungen
- Psych DrugsDokument12 SeitenPsych Drugsapi-3739910100% (1)
- Table 1: Patient's Response On The Effectiveness of The Aratiles Leaves TeaDokument11 SeitenTable 1: Patient's Response On The Effectiveness of The Aratiles Leaves TeaAlice Del Rosario CabanaNoch keine Bewertungen
- Tabel Obat Kardiovaskuler Aulia Nurtafani Reforma (189296)Dokument9 SeitenTabel Obat Kardiovaskuler Aulia Nurtafani Reforma (189296)Aulia Nurtafani ReformaNoch keine Bewertungen
- Tablet Coating BasicsDokument4 SeitenTablet Coating BasicsTahir KhanNoch keine Bewertungen