Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Crystal Growth ProjectDokument47 SeitenCrystal Growth ProjectVIJEESH P100% (2)
- Arlamol LST DS-295-5 PDFDokument12 SeitenArlamol LST DS-295-5 PDFsimmiNoch keine Bewertungen
- Solution - Colligative Properties Exercise PDFDokument27 SeitenSolution - Colligative Properties Exercise PDFGOURISH AGRAWALNoch keine Bewertungen
- The Cyanide Process of Gold Extraction 1000740146 PDFDokument260 SeitenThe Cyanide Process of Gold Extraction 1000740146 PDFAnonymous rBcspMzPNoch keine Bewertungen
- Sugar Factory DefinitionDokument8 SeitenSugar Factory Definitiontsrinivasan5083100% (1)
- Durability of Clay Brick Masonry Walls Reviewed for Salt AttackDokument18 SeitenDurability of Clay Brick Masonry Walls Reviewed for Salt AttackKizito NathanNoch keine Bewertungen
- To Paste Nov8Dokument194 SeitenTo Paste Nov8Jerome Rivera CastroNoch keine Bewertungen
- IGCSE EdExcel 9 1 Chemistry Topic 1 Principles of ChemistryDokument115 SeitenIGCSE EdExcel 9 1 Chemistry Topic 1 Principles of ChemistryRobnawaz KhanNoch keine Bewertungen
- Overlord v13 c2 + Intermission All Parts EnglishDokument85 SeitenOverlord v13 c2 + Intermission All Parts EnglishJerome Rivera CastroNoch keine Bewertungen
- Traffic OverviewDokument2 SeitenTraffic OverviewJerome Rivera CastroNoch keine Bewertungen
- Overlord v13 c1 All Parts EnglishDokument86 SeitenOverlord v13 c1 All Parts EnglishJerome Rivera CastroNoch keine Bewertungen
- Performance Report For:: Executive SummaryDokument23 SeitenPerformance Report For:: Executive SummaryJerome Rivera CastroNoch keine Bewertungen
- CLE I Semifinal Test GabDokument2 SeitenCLE I Semifinal Test GabJerome Rivera CastroNoch keine Bewertungen
- Philo Homework Aug 17Dokument3 SeitenPhilo Homework Aug 17Jerome Rivera CastroNoch keine Bewertungen
- b09 1414 PDFDokument8 Seitenb09 1414 PDFJerome Rivera CastroNoch keine Bewertungen
- HomeworksDokument6 SeitenHomeworksJerome Rivera CastroNoch keine Bewertungen
- Overlord Volume 12 - The Paladin of The Holy Kingdom - Black EditionDokument398 SeitenOverlord Volume 12 - The Paladin of The Holy Kingdom - Black EditionJerome Rivera CastroNoch keine Bewertungen
- Philo Homework Aug 17Dokument3 SeitenPhilo Homework Aug 17Jerome Rivera CastroNoch keine Bewertungen
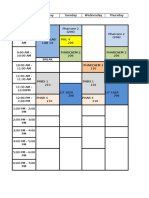
- Steph Sked Sem 1 2016Dokument2 SeitenSteph Sked Sem 1 2016Jerome Rivera CastroNoch keine Bewertungen
- Biochem Structures and FunctionsDokument7 SeitenBiochem Structures and FunctionsJerome Rivera CastroNoch keine Bewertungen
- Three Letter Abbrevi Ation Line-Dash ModelDokument11 SeitenThree Letter Abbrevi Ation Line-Dash ModelJerome Rivera CastroNoch keine Bewertungen
- AntifungalsDokument1 SeiteAntifungalsJerome Rivera CastroNoch keine Bewertungen
- 36" Single RX Metal Bay Unit - 329 USDDokument5 Seiten36" Single RX Metal Bay Unit - 329 USDJerome Rivera CastroNoch keine Bewertungen
- ReflexesDokument1 SeiteReflexesJerome Rivera CastroNoch keine Bewertungen
- HospitalsDokument1 SeiteHospitalsJerome Rivera CastroNoch keine Bewertungen
- Anatomy of The EyeDokument3 SeitenAnatomy of The EyeJerome Rivera CastroNoch keine Bewertungen
- Table TennisDokument18 SeitenTable TennisJoslin RozNoch keine Bewertungen
- Auditory Pathway PDFDokument35 SeitenAuditory Pathway PDFJohnson JayarajNoch keine Bewertungen
- Experiment 8Dokument1 SeiteExperiment 8Jerome Rivera CastroNoch keine Bewertungen
- Magmas and Gels: Dr. Mehwish Qayyum Pharm.d Ms - Drug Design and Discovery (University of Surrey) Senior LecturerDokument22 SeitenMagmas and Gels: Dr. Mehwish Qayyum Pharm.d Ms - Drug Design and Discovery (University of Surrey) Senior LecturerJerome Rivera CastroNoch keine Bewertungen
- SuppositoriesDokument3 SeitenSuppositoriesJerome Rivera CastroNoch keine Bewertungen
- AlaaDokument1 SeiteAlaaJerome Rivera CastroNoch keine Bewertungen
- Experiment 8Dokument1 SeiteExperiment 8Jerome Rivera CastroNoch keine Bewertungen
- Transdermal SDokument5 SeitenTransdermal SJerome Rivera CastroNoch keine Bewertungen
- Location List+Evolution NotesDokument9 SeitenLocation List+Evolution NotesJerome Rivera CastroNoch keine Bewertungen
- FAQ and Known BugsDokument3 SeitenFAQ and Known BugsJerome Rivera CastroNoch keine Bewertungen
- LiberationDokument33 SeitenLiberationAnthony Catapang PascualNoch keine Bewertungen
- 1 - Informações Completas HOPZOILDokument2 Seiten1 - Informações Completas HOPZOILMario E. M. BitencourtNoch keine Bewertungen
- Paper 3 June 1999Dokument4 SeitenPaper 3 June 1999MSHNoch keine Bewertungen
- Questions About DensityDokument8 SeitenQuestions About DensityJohn OsborneNoch keine Bewertungen
- CurcuminDokument8 SeitenCurcuminRizki Septiani YuarsaNoch keine Bewertungen
- Polymer Chemistry PDFDokument31 SeitenPolymer Chemistry PDFSiti Nurul ShahidaNoch keine Bewertungen
- Earth and Planetary Science Letters: Robert C. Newton, Craig E. ManningDokument9 SeitenEarth and Planetary Science Letters: Robert C. Newton, Craig E. Manningarkan ayatullohNoch keine Bewertungen
- Water Content of The Kawah Kamojang Geothermal ReservoirDokument10 SeitenWater Content of The Kawah Kamojang Geothermal ReservoirAswar Abu KhawlahNoch keine Bewertungen
- (PVA) Physical and Mechanical Properties of Water Resistant PDFDokument8 Seiten(PVA) Physical and Mechanical Properties of Water Resistant PDFCarolina AyalaNoch keine Bewertungen
- Chem 1010 Lab ManualDokument141 SeitenChem 1010 Lab ManualRaina IslamNoch keine Bewertungen
- January 2020 Chemistry Mark Scheme 2CDokument7 SeitenJanuary 2020 Chemistry Mark Scheme 2CMeenakshie Chaudrie0% (1)
- CHE 435 Liquid-Liquid Extraction Lab ManualDokument24 SeitenCHE 435 Liquid-Liquid Extraction Lab ManualStolen RememberNoch keine Bewertungen
- Hort382 PDFDokument123 SeitenHort382 PDFUdayabhanu AngirekulaNoch keine Bewertungen
- Keroflux 6238 - TDSDokument2 SeitenKeroflux 6238 - TDSExtrovertido Sin LimitesNoch keine Bewertungen
- Chemistry Solutions For Pretrucci's Book ChemistryDokument56 SeitenChemistry Solutions For Pretrucci's Book ChemistryDonnie George0% (1)
- DisoluciónDokument8 SeitenDisoluciónJesús Salomón Bárcenas HernándezNoch keine Bewertungen
- Solutions and Solubility ExplainedDokument64 SeitenSolutions and Solubility ExplainedSohila A. MabroukNoch keine Bewertungen
- A Comparative Chemical Analytical Study of Mercuric Chloride (Veeram) On Before and After PurificationDokument7 SeitenA Comparative Chemical Analytical Study of Mercuric Chloride (Veeram) On Before and After Purificationjmanuel108yahoo.co.ukNoch keine Bewertungen
- Qualitative Physicochemical, Phytochemical Analysis and Quantitative Estimation of Total Phenols, Flavonoids and Alkaloids of Boerhaavia DiffusaDokument10 SeitenQualitative Physicochemical, Phytochemical Analysis and Quantitative Estimation of Total Phenols, Flavonoids and Alkaloids of Boerhaavia DiffusaDr. Ramadevi DevarakondaNoch keine Bewertungen
- Hot-Melt Extrusion Microencapsulation of Quercetin For Taste-Masking.Dokument10 SeitenHot-Melt Extrusion Microencapsulation of Quercetin For Taste-Masking.Chus Otto BellostaNoch keine Bewertungen
- CHM303LAB1Dokument7 SeitenCHM303LAB1Darvin YiNoch keine Bewertungen
- FAST Scale Course Background and PredictionDokument103 SeitenFAST Scale Course Background and PredictionGeorge Zabaras100% (1)
- 7.3 Salt Preparation PPQ - SDokument10 Seiten7.3 Salt Preparation PPQ - SWu YiruiNoch keine Bewertungen