Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Medical TerminologyDokument103 SeitenMedical Terminologyrockinqueenful100% (15)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Single Best Answer (SBA) QuestionsDokument16 SeitenSingle Best Answer (SBA) QuestionsKrairat Komdee50% (2)
- Molecular Etiopathogenesis of Ameloblastoma CurrentDokument5 SeitenMolecular Etiopathogenesis of Ameloblastoma CurrentRiskha Febriani HapsariNoch keine Bewertungen
- Skippers United Pacific, Inc. vs. Lagne DigestDokument4 SeitenSkippers United Pacific, Inc. vs. Lagne DigestEmir MendozaNoch keine Bewertungen
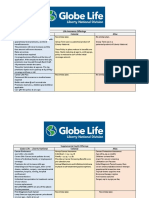
- Life Insurance Offerings Globe Life - Liberty National Colonial AflacDokument3 SeitenLife Insurance Offerings Globe Life - Liberty National Colonial AflacTina Hughes0% (1)
- HypothyroidismDokument146 SeitenHypothyroidismAisha Wadiwala100% (1)
- CANCER - Ayurvedic ApproachDokument6 SeitenCANCER - Ayurvedic ApproachAnonymous L85tmrUnNoch keine Bewertungen
- Orh Figure7 PDFDokument1 SeiteOrh Figure7 PDFRiskha Febriani HapsariNoch keine Bewertungen
- Third MolarDokument6 SeitenThird MolarRiskha Febriani HapsariNoch keine Bewertungen
- Adjuncts To Local AnesthesiaDokument10 SeitenAdjuncts To Local AnesthesiaRiskha Febriani HapsariNoch keine Bewertungen
- The Endocrine Society Clinical Practice Guidelines: A Self-AssessmentDokument4 SeitenThe Endocrine Society Clinical Practice Guidelines: A Self-AssessmentRiskha Febriani HapsariNoch keine Bewertungen
- A Review of Surface Treatment Methods To Improve The Adhesive Cementation of Zirconia-Based CeramicsDokument11 SeitenA Review of Surface Treatment Methods To Improve The Adhesive Cementation of Zirconia-Based CeramicsRiskha Febriani HapsariNoch keine Bewertungen
- Etiology MaloclusionDokument3 SeitenEtiology MaloclusionRiskha Febriani HapsariNoch keine Bewertungen
- Profile Changes in Premolar Extraction: Alterações No Perfil em Extrações de Pré-MolaresDokument7 SeitenProfile Changes in Premolar Extraction: Alterações No Perfil em Extrações de Pré-MolaresRiskha Febriani HapsariNoch keine Bewertungen
- Abjna 3 2 43 48Dokument6 SeitenAbjna 3 2 43 48Riskha Febriani HapsariNoch keine Bewertungen
- Drug Study SittieDokument8 SeitenDrug Study SittieHarrisha G SanduyoganNoch keine Bewertungen
- BRVO PPT by Dr. Chinmay KharadeDokument31 SeitenBRVO PPT by Dr. Chinmay KharadeChinmay KharadeNoch keine Bewertungen
- Medicographia115 PDFDokument119 SeitenMedicographia115 PDFRafael CastilloNoch keine Bewertungen
- Vitamins + Their DeficienciesDokument6 SeitenVitamins + Their DeficienciesKieran KillingtonNoch keine Bewertungen
- Anti-Inflammatory Effect of Panyawan Stem For Toothache (1)Dokument10 SeitenAnti-Inflammatory Effect of Panyawan Stem For Toothache (1)Nolemae NavalesNoch keine Bewertungen
- Matary Appendix Summary01Dokument4 SeitenMatary Appendix Summary01Muhammad GoharNoch keine Bewertungen
- Monitoring and Evaluation of Health Services: Dr. Rasha SalamaDokument52 SeitenMonitoring and Evaluation of Health Services: Dr. Rasha SalamaLibyaFlowerNoch keine Bewertungen
- JaundiceDokument6 SeitenJaundiceNiaNoch keine Bewertungen
- Chapter 22 - The Respiratory SystemDokument15 SeitenChapter 22 - The Respiratory SystemTony Snearly100% (1)
- Clinical Atlas of Canine and Feline Dermatology - 2019 - Coyner - IndexDokument12 SeitenClinical Atlas of Canine and Feline Dermatology - 2019 - Coyner - Indexnabal22Noch keine Bewertungen
- Alcoholic Liver Disease PDFDokument13 SeitenAlcoholic Liver Disease PDFPrabhakaran ganjuNoch keine Bewertungen
- El Cuidado de Mother Teresa de Los Moribundos - 1994 - The LANCET - ScienceDirectDokument1 SeiteEl Cuidado de Mother Teresa de Los Moribundos - 1994 - The LANCET - ScienceDirectCarlosYovadSaldamandoCruzNoch keine Bewertungen
- MC0620179970 HDFC Life Group Credit Protect PlusDokument8 SeitenMC0620179970 HDFC Life Group Credit Protect PlusAditya RajNoch keine Bewertungen
- CA Oral CavityDokument53 SeitenCA Oral Cavityaakash11Noch keine Bewertungen
- DAFTAR PUSTAKA AripinDokument2 SeitenDAFTAR PUSTAKA AripinFerdy Ricardo SinagaNoch keine Bewertungen
- Intermittent Vs Indwelling CatheterizationDokument2 SeitenIntermittent Vs Indwelling CatheterizationWildan DzakiyNoch keine Bewertungen
- University College London Medical School (Ucl) : 2-Year Academic Foundation Programmes atDokument16 SeitenUniversity College London Medical School (Ucl) : 2-Year Academic Foundation Programmes atPaul CarterNoch keine Bewertungen
- Untitled 1Dokument17 SeitenUntitled 1Tiberiu CttNoch keine Bewertungen
- Candidate'S Biodata: Project Code: Project Title: A. Personal DataDokument7 SeitenCandidate'S Biodata: Project Code: Project Title: A. Personal DataAmazing and FunnyNoch keine Bewertungen
- Achalasia: A Review of Etiology, Pathophysiology, and TreatmentDokument6 SeitenAchalasia: A Review of Etiology, Pathophysiology, and TreatmentAprita NurkarimaNoch keine Bewertungen
- Left Thigh Pain: I. Chief Complaint/ Other ComplaintsDokument9 SeitenLeft Thigh Pain: I. Chief Complaint/ Other ComplaintsDominic BristolNoch keine Bewertungen
- Heterotopic Bone Formation Final Draft-ZemenfesDokument5 SeitenHeterotopic Bone Formation Final Draft-Zemenfesapi-270166097Noch keine Bewertungen
- Dysgeusia PDFDokument3 SeitenDysgeusia PDFErika DiannaNoch keine Bewertungen
- LDN (Low Dose Naltrexone) VariousPatentsandPatentApplicationsDokument47 SeitenLDN (Low Dose Naltrexone) VariousPatentsandPatentApplicationsLynn Allison NelsonNoch keine Bewertungen