Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Ron Kurtz - The Body Reveals PDFDokument161 SeitenRon Kurtz - The Body Reveals PDFNemanja92% (12)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Biology PDFDokument1.447 SeitenBiology PDFPrincess Ethel Atillo100% (2)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- How To Get TallerDokument71 SeitenHow To Get TallerH0X3M4G1C0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Come Thirsty Chapter1Dokument4 SeitenCome Thirsty Chapter1Natalia Lupasco100% (1)
- How Can We Use Neurotransmitters in Emotion and Reward System To Study DepressionDokument22 SeitenHow Can We Use Neurotransmitters in Emotion and Reward System To Study DepressionGlobal Research and Development ServicesNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Pharmacology Nursing ReviewDokument19 SeitenPharmacology Nursing Reviewp_dawg50% (2)
- Abdominal SurgeryDokument166 SeitenAbdominal SurgeryIndera VyasNoch keine Bewertungen
- ICSE Class 10 Biology Previous Year Question Paper 2011 PDFDokument9 SeitenICSE Class 10 Biology Previous Year Question Paper 2011 PDFmohammedNoch keine Bewertungen
- Nervous System - All NotesDokument6 SeitenNervous System - All NotesJNoch keine Bewertungen
- Refeeding SyndromeDokument4 SeitenRefeeding SyndromeallyNoch keine Bewertungen
- Brainstem Bravo AnnotatedDokument13 SeitenBrainstem Bravo AnnotatedMia CadizNoch keine Bewertungen
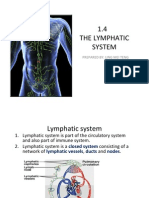
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDokument15 Seiten1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNoch keine Bewertungen
- Lipid Membrane Composition and SignificanceDokument4 SeitenLipid Membrane Composition and SignificanceZainab AliNoch keine Bewertungen
- Arthropod-Plant Interactions Novel Insights and Approaches For IPMDokument238 SeitenArthropod-Plant Interactions Novel Insights and Approaches For IPMAnonymous T9uyM2Noch keine Bewertungen
- The Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Dokument10 SeitenThe Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Miguel Angel Quiroz CristobalNoch keine Bewertungen
- Mechanisms of Cardiac Arrhythmias From Automatici+Dokument24 SeitenMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanNoch keine Bewertungen
- B CellDokument10 SeitenB CellSonia Elizabeth SimonNoch keine Bewertungen
- C5 - Metabolism and Enzyme Part 1Dokument20 SeitenC5 - Metabolism and Enzyme Part 1Daniel LohNoch keine Bewertungen
- Biology #KautilyaDokument79 SeitenBiology #KautilyapankajNoch keine Bewertungen
- The Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Dokument5 SeitenThe Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Sinem SerapNoch keine Bewertungen
- Altered Body TemperatureDokument27 SeitenAltered Body TemperatureAnusikta PandaNoch keine Bewertungen
- CHAPTER SUMMARY-opiod AnalgesicDokument9 SeitenCHAPTER SUMMARY-opiod AnalgesicNuttiya WerawattanachaiNoch keine Bewertungen
- Risk For Decreased Cardiac OutputDokument4 SeitenRisk For Decreased Cardiac Outputapi-283482759Noch keine Bewertungen
- Traumatic Hyphema PDFDokument10 SeitenTraumatic Hyphema PDFPratiwi SimanNoch keine Bewertungen
- MSC 060913 PDFDokument44 SeitenMSC 060913 PDFViroopaksha V JaddipalNoch keine Bewertungen
- Bacillus lipopeptides: versatile weapons against plant diseasesDokument11 SeitenBacillus lipopeptides: versatile weapons against plant diseasesjazminNoch keine Bewertungen
- SP FinalDokument18 SeitenSP Finalapi-344954734Noch keine Bewertungen
- AP PSYCHOLOGY EXAM REVIEW SHEETDokument6 SeitenAP PSYCHOLOGY EXAM REVIEW SHEETNathan HudsonNoch keine Bewertungen
- Animal Morphology (GeoZoo Topics)Dokument5 SeitenAnimal Morphology (GeoZoo Topics)niravhirparaNoch keine Bewertungen
- Comprehensive Review of Temporal Lobe EpilepsyDokument36 SeitenComprehensive Review of Temporal Lobe Epilepsyyohanes0gadiNoch keine Bewertungen