Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Development of The Face 2015 PDFDokument2 SeitenDevelopment of The Face 2015 PDFAnny AlvrzNoch keine Bewertungen
- Topic Breakdown 2nd Year First SemDokument6 SeitenTopic Breakdown 2nd Year First SemAnny AlvrzNoch keine Bewertungen
- Histology of Ear and EyeDokument2 SeitenHistology of Ear and EyeAnny Alvrz100% (1)
- Biology AssignmentDokument3 SeitenBiology AssignmentAnny AlvrzNoch keine Bewertungen
- Ears and EyesDokument4 SeitenEars and EyesAnny AlvrzNoch keine Bewertungen
- Prepare For The End Time Move of The Holy Spirit Jesus Is Coming Again Apostle Abraham JCBC 101415Dokument57 SeitenPrepare For The End Time Move of The Holy Spirit Jesus Is Coming Again Apostle Abraham JCBC 101415Anny AlvrzNoch keine Bewertungen
- Love Your GardenDokument17 SeitenLove Your GardenAnny AlvrzNoch keine Bewertungen
- Utilizing PKPD To Optimize TherapyDokument39 SeitenUtilizing PKPD To Optimize TherapyAnny AlvrzNoch keine Bewertungen
- Cranial Nerves and Their Sensory Association NeuronsDokument3 SeitenCranial Nerves and Their Sensory Association NeuronsAnny AlvrzNoch keine Bewertungen
- Obedience Is The Key To Unlock Your MiraclesDokument11 SeitenObedience Is The Key To Unlock Your MiraclesAnny AlvrzNoch keine Bewertungen
- Biofemme ICONDokument34 SeitenBiofemme ICONAnny AlvrzNoch keine Bewertungen
- Filipino Family: Marthony P. Basco, MD, MPH DCFM - Feu, NRMFDokument10 SeitenFilipino Family: Marthony P. Basco, MD, MPH DCFM - Feu, NRMFAnny AlvrzNoch keine Bewertungen
- Optimizing and Maximizing Antibiotic TherapyDokument76 SeitenOptimizing and Maximizing Antibiotic TherapyAnny AlvrzNoch keine Bewertungen
- You Have The Power To Believe SignsDokument18 SeitenYou Have The Power To Believe SignsAnny AlvrzNoch keine Bewertungen
- You Can Be VictoriousDokument1 SeiteYou Can Be VictoriousAnny AlvrzNoch keine Bewertungen
- Build Your Garden To Be A Witness of God's FaithfulnessDokument18 SeitenBuild Your Garden To Be A Witness of God's FaithfulnessAnny AlvrzNoch keine Bewertungen
- How To Beautify and Maintain Your Garden in The Power of The Holy SpiritDokument28 SeitenHow To Beautify and Maintain Your Garden in The Power of The Holy SpiritAnny AlvrzNoch keine Bewertungen
- Autonomy & JusticeDokument4 SeitenAutonomy & JusticeAnny AlvrzNoch keine Bewertungen
- (BiochemB) Signal Transduction - Dr. Viliran (Bernabe and Dela Rosa) PDFDokument13 Seiten(BiochemB) Signal Transduction - Dr. Viliran (Bernabe and Dela Rosa) PDFAnny AlvrzNoch keine Bewertungen
- You Are Not A FailureDokument17 SeitenYou Are Not A FailureAnny AlvrzNoch keine Bewertungen
- Scalp Gross AnatomyDokument5 SeitenScalp Gross AnatomyAnny AlvrzNoch keine Bewertungen
- CSF and Ventricular SystemDokument24 SeitenCSF and Ventricular SystemAnny AlvrzNoch keine Bewertungen
- Four Principles Approach To EthicsDokument5 SeitenFour Principles Approach To EthicsAnny AlvrzNoch keine Bewertungen
- Believe Signs and Wonders and MiraclesDokument12 SeitenBelieve Signs and Wonders and MiraclesAnny AlvrzNoch keine Bewertungen
- CFM I Physical Activity GuicoDokument7 SeitenCFM I Physical Activity GuicoAnny AlvrzNoch keine Bewertungen
- Waste Management: Louricha A. Opina-Tan, MD Department of Community and Family MedicineDokument34 SeitenWaste Management: Louricha A. Opina-Tan, MD Department of Community and Family MedicineAnny AlvrzNoch keine Bewertungen
- Tools in Family AssessmentDokument3 SeitenTools in Family AssessmentAnny Alvrz83% (6)
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDokument5 SeitenPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzNoch keine Bewertungen
- Anterior and Posterio Pituitary GlandDokument7 SeitenAnterior and Posterio Pituitary GlandAnny AlvrzNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDokument20 SeitenDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNoch keine Bewertungen
- AntibioticsDokument9 SeitenAntibiotics7aith22Noch keine Bewertungen
- Tetracycline's: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeDokument21 SeitenTetracycline's: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeJagirNoch keine Bewertungen
- 6-Protein Synthesis InhibitorDokument71 Seiten6-Protein Synthesis InhibitorAlexa Joy InguilloNoch keine Bewertungen
- Discromii 1Dokument4 SeitenDiscromii 1defineyoung5Noch keine Bewertungen
- Tigecycline Alone or in CombinationDokument13 SeitenTigecycline Alone or in CombinationSanjay NavaleNoch keine Bewertungen
- PharmaAntianginal DrugsDokument175 SeitenPharmaAntianginal DrugsNidal AbboudNoch keine Bewertungen
- Sun 2015Dokument10 SeitenSun 2015sarah assegafNoch keine Bewertungen
- Naplex Infectiious Disease QuestionsDokument4 SeitenNaplex Infectiious Disease QuestionsSARANYANoch keine Bewertungen
- Antifungal Agents: LipopeptidesDokument8 SeitenAntifungal Agents: LipopeptidesCristian QuitoNoch keine Bewertungen
- Evaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsDokument8 SeitenEvaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsRicardo ZúñigaNoch keine Bewertungen
- Drug Bug TableDokument1 SeiteDrug Bug TableLes SangaNoch keine Bewertungen
- Basic Clinical Pharmacology 14th Edition McGraw Hill Education Bertram G. Katzung 2017 829 847Dokument19 SeitenBasic Clinical Pharmacology 14th Edition McGraw Hill Education Bertram G. Katzung 2017 829 847Faye Kashmier Embestro NamoroNoch keine Bewertungen
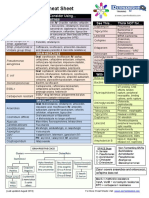
- Antibiotic Study Cheat Sheet August 2019Dokument1 SeiteAntibiotic Study Cheat Sheet August 2019Ryan TurnerNoch keine Bewertungen
- AntibioticsDokument17 SeitenAntibioticsnehal.nehal92Noch keine Bewertungen
- Antibiotic Optimization in CIAIDokument33 SeitenAntibiotic Optimization in CIAIAditya Pradana KNoch keine Bewertungen
- Microbewiki - Kenyon.edu Index - PHP Enterobacter CloacaeDokument4 SeitenMicrobewiki - Kenyon.edu Index - PHP Enterobacter Cloacaehari.suryanto8417Noch keine Bewertungen
- Medmastery Antimicrobial - Stewardship - HandbookDokument65 SeitenMedmastery Antimicrobial - Stewardship - HandbookHhaNoch keine Bewertungen
- Antibiotic Resistance in Diabetic Foot Soft Tissue Infections: A Series From GreeceDokument5 SeitenAntibiotic Resistance in Diabetic Foot Soft Tissue Infections: A Series From GreeceBelinda AngelNoch keine Bewertungen
- Guias Infecciones Intraabdominales IdsaDokument32 SeitenGuias Infecciones Intraabdominales IdsaSylvain ColluraNoch keine Bewertungen
- 31041313Dokument10 Seiten31041313carolinapolotorresNoch keine Bewertungen
- Antibiotics For PneumoniaDokument52 SeitenAntibiotics For PneumoniaAndy DazNoch keine Bewertungen
- Tigecycline Antibacterial Activity, Clinical Effectiveness, and Mechanisms and Epidemiology of ResistanceDokument20 SeitenTigecycline Antibacterial Activity, Clinical Effectiveness, and Mechanisms and Epidemiology of ResistanceDanielle pfizerNoch keine Bewertungen
- Newer Antibiotics: Guide: DR Saroja A ODokument51 SeitenNewer Antibiotics: Guide: DR Saroja A OparahulNoch keine Bewertungen
- Guoying Wang, Guo ZhaoDokument17 SeitenGuoying Wang, Guo ZhaoHQ HQNoch keine Bewertungen
- Chapter 043Dokument6 SeitenChapter 043borisdevic223Noch keine Bewertungen
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Dokument12 SeitenIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNoch keine Bewertungen
- 6811 PDFDokument11 Seiten6811 PDFMaileth Carolina Anillo ArrietaNoch keine Bewertungen
- Artigo Produtos NaturaisDokument39 SeitenArtigo Produtos NaturaisMillygoNoch keine Bewertungen
- Drug of Choices PDFDokument10 SeitenDrug of Choices PDFRavi Amin100% (1)