Das könnte Ihnen auch gefallen
- Harrison TablesDokument163 SeitenHarrison Tablesfrancieudo1Noch keine Bewertungen
- Parasites of Medical ImportanceDokument9 SeitenParasites of Medical ImportanceKimberly RampersadNoch keine Bewertungen
- Seminar2saliva 160425090015 PDFDokument101 SeitenSeminar2saliva 160425090015 PDFYus Arlika Putra WibawaNoch keine Bewertungen
- Genetics and Epigenetics of Infertility and Treatments On OutcomesDokument16 SeitenGenetics and Epigenetics of Infertility and Treatments On OutcomesCamii Cv100% (1)
- Hematology Report:: Lahore: 07 Jail Road, Main Gulberg - Karachi: Al Khaleej Plaza, Shaheed-e-Millat RoadDokument2 SeitenHematology Report:: Lahore: 07 Jail Road, Main Gulberg - Karachi: Al Khaleej Plaza, Shaheed-e-Millat RoadAliNoch keine Bewertungen
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeVon EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNoch keine Bewertungen
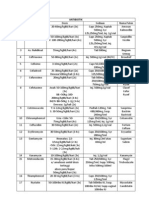
- Daftar Dosis Dan Sediaan ObatDokument5 SeitenDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- Daftar Dosis Dan Sediaan ObatDokument5 SeitenDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- Daftar Dosis Dan Sediaan ObatDokument5 SeitenDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- BookDokument38 SeitenBookAlleah Mancilla100% (1)
- Schistosomiasis Case StudyDokument5 SeitenSchistosomiasis Case Studyapi-318749549Noch keine Bewertungen
- Recurrent Hypertensive Disease Associated With Increased Long-Term Mortality RisksDokument6 SeitenRecurrent Hypertensive Disease Associated With Increased Long-Term Mortality RisksNandina Rosa FloridanaNoch keine Bewertungen
- Lower Perineal Trauma Risk for Stillbirth DeliveriesDokument5 SeitenLower Perineal Trauma Risk for Stillbirth DeliveriesSy Yessy ParamitaNoch keine Bewertungen
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDokument6 SeitenAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNoch keine Bewertungen
- CDC 84627 DS1Dokument15 SeitenCDC 84627 DS1Thu HoaiNoch keine Bewertungen
- Women's Health Care Physicians: Member Login Join Pay Dues Follow UsDokument24 SeitenWomen's Health Care Physicians: Member Login Join Pay Dues Follow UsNazif Aiman IsmailNoch keine Bewertungen
- BanhartDokument8 SeitenBanhartshaNoch keine Bewertungen
- History of Indiced AbortionDokument8 SeitenHistory of Indiced AbortionSalsabila AjengNoch keine Bewertungen
- Pregnancy-Induced Hypertension Is An Independent Risk Factor For Meconium Aspiration Syndrome A Retrospective Population Based Cohort StudyDokument5 SeitenPregnancy-Induced Hypertension Is An Independent Risk Factor For Meconium Aspiration Syndrome A Retrospective Population Based Cohort StudyRIECHELLE SEVILLANoch keine Bewertungen
- Artigo 3Dokument7 SeitenArtigo 3Cirineu NetoNoch keine Bewertungen
- Articulo 5Dokument6 SeitenArticulo 5Monica ReyesNoch keine Bewertungen
- Changed Indications For Cesarean Sections: Ylva Vladic Stjernholm, Karin Petersson & Eva EnerothDokument5 SeitenChanged Indications For Cesarean Sections: Ylva Vladic Stjernholm, Karin Petersson & Eva EnerothSam Ath SanNoch keine Bewertungen
- Sayar, 2011Dokument6 SeitenSayar, 2011Cristina CarpioNoch keine Bewertungen
- Poster Session V Highlights Risks of Cesarean Deliveries and Optimal Management of Postterm PregnanciesDokument1 SeitePoster Session V Highlights Risks of Cesarean Deliveries and Optimal Management of Postterm PregnanciesniluhNoch keine Bewertungen
- 1 s2.0 S1028455919300178 Main PDFDokument5 Seiten1 s2.0 S1028455919300178 Main PDFRadinal PrayitnoNoch keine Bewertungen
- Del 153Dokument6 SeitenDel 153Fan AccountNoch keine Bewertungen
- Acute Pyelonephritis in PregnancyDokument7 SeitenAcute Pyelonephritis in PregnancyKvmLlyNoch keine Bewertungen
- Winter, Spring, Summer or Fall Temporal Patterns in Placenta-Mediated Pregnancy Complications-An Exploratory AnalysisDokument8 SeitenWinter, Spring, Summer or Fall Temporal Patterns in Placenta-Mediated Pregnancy Complications-An Exploratory AnalysisTushar RameshNoch keine Bewertungen
- Am J Perinatol. 2007 Jun24 (6) 373-6Dokument4 SeitenAm J Perinatol. 2007 Jun24 (6) 373-6Ivan Osorio RuizNoch keine Bewertungen
- None 3Dokument7 SeitenNone 3Sy Yessy ParamitaNoch keine Bewertungen
- Altered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVDokument17 SeitenAltered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVMuhammad Pebri Nilhakim ZavbmNoch keine Bewertungen
- Chouinard2019 PDFDokument8 SeitenChouinard2019 PDFanggunNoch keine Bewertungen
- Selected Pregnancy and Perinatal Outcomes of Patients With and Without A Previous Placenta AccreteDokument2 SeitenSelected Pregnancy and Perinatal Outcomes of Patients With and Without A Previous Placenta AccreteMuhammad IkbarNoch keine Bewertungen
- Morbilidad Y Mortalidad Materna Y Perinatal de La Diabetes Gestacional en Una Población MexicanaDokument11 SeitenMorbilidad Y Mortalidad Materna Y Perinatal de La Diabetes Gestacional en Una Población MexicanaEnith Perez RangelNoch keine Bewertungen
- Journal (Preterm Labor)Dokument5 SeitenJournal (Preterm Labor)Zhyraine Iraj D. CaluzaNoch keine Bewertungen
- Platelet Count in First Trimester of Pregnancy As Apredictor of Perinatal OutcomeDokument6 SeitenPlatelet Count in First Trimester of Pregnancy As Apredictor of Perinatal OutcomececilliacynthiaNoch keine Bewertungen
- Prolonged Pregnancy: When Should We InterveneDokument11 SeitenProlonged Pregnancy: When Should We InterveneRaul DoctoNoch keine Bewertungen
- Jurnal Abrupsio PlasentaDokument13 SeitenJurnal Abrupsio Plasentaperussi pranadiptaNoch keine Bewertungen
- Jurnal 1 MaterDokument4 SeitenJurnal 1 MaterEvaliaRahmatPuzianNoch keine Bewertungen
- Keeling 2019Dokument8 SeitenKeeling 2019senkonenNoch keine Bewertungen
- PIIS2210778916303701Dokument2 SeitenPIIS2210778916303701Fatimah AssagafNoch keine Bewertungen
- $116 SMFM AbstractsDokument1 Seite$116 SMFM AbstractsSheila Regina TizaNoch keine Bewertungen
- Safe Prevention of The Primary Cesarean Delivery - ACOGDokument16 SeitenSafe Prevention of The Primary Cesarean Delivery - ACOGAryaNoch keine Bewertungen
- Hum. Reprod. 2012 Velez Edwards 54-60-2Dokument7 SeitenHum. Reprod. 2012 Velez Edwards 54-60-2Putri Nilam SariNoch keine Bewertungen
- Rethinking IUGR in preeclampsiaDokument5 SeitenRethinking IUGR in preeclampsiaAntonius Joko NugrohoNoch keine Bewertungen
- Thyroid and Pregnancy OutcomeDokument9 SeitenThyroid and Pregnancy OutcomeCindy KestyNoch keine Bewertungen
- AbruptionDokument13 SeitenAbruptionMauricio Lopez MejiaNoch keine Bewertungen
- The Effects of Threatened Abortions On Pregnancy OutcomesDokument6 SeitenThe Effects of Threatened Abortions On Pregnancy OutcomesfrankyNoch keine Bewertungen
- Research Article: Pregnancy Outcome of Multiparous Women Aged Over 40 YearsDokument4 SeitenResearch Article: Pregnancy Outcome of Multiparous Women Aged Over 40 YearsChristine Laurenza SNoch keine Bewertungen
- Periodontal Infection and Preterm Birth: Results of A Prospective StudyDokument6 SeitenPeriodontal Infection and Preterm Birth: Results of A Prospective StudypetrarizkyNoch keine Bewertungen
- Maternal and Obstetric Outcome of Women With Epilepsy 2009 SeizureDokument4 SeitenMaternal and Obstetric Outcome of Women With Epilepsy 2009 Seizurebilal hadiNoch keine Bewertungen
- Prolonged Second Stage of Labour, Maternal Infectious Disease, Urinary Retention and Other Complications in The Early Postpartum PeriodDokument9 SeitenProlonged Second Stage of Labour, Maternal Infectious Disease, Urinary Retention and Other Complications in The Early Postpartum PeriodCordova ArridhoNoch keine Bewertungen
- Bad Obstetric History and Infectious CausesDokument3 SeitenBad Obstetric History and Infectious Causeskyle31Noch keine Bewertungen
- Acute Pyelonephritis During Pregnancy: A Systematic Review of The Aetiology, Timing, and Reported Adverse Perinatal Risks During PregnancyDokument11 SeitenAcute Pyelonephritis During Pregnancy: A Systematic Review of The Aetiology, Timing, and Reported Adverse Perinatal Risks During PregnancyRahul DhulipalaNoch keine Bewertungen
- Preterm Premature Rupture of Membranes in The Presence of Cerclage: Is The Risk For Intra-Uterine Infection and Adverse Neonatal Outcome Increased?Dokument6 SeitenPreterm Premature Rupture of Membranes in The Presence of Cerclage: Is The Risk For Intra-Uterine Infection and Adverse Neonatal Outcome Increased?stephaniedianNoch keine Bewertungen
- Placenta PreviaDokument5 SeitenPlacenta PreviaKuro HanabusaNoch keine Bewertungen
- Herrera 2017Dokument9 SeitenHerrera 2017Bianca Maria PricopNoch keine Bewertungen
- PIIS0002937821019992Dokument2 SeitenPIIS0002937821019992made dharmaNoch keine Bewertungen
- Original ContributionDokument10 SeitenOriginal ContributionzzakieNoch keine Bewertungen
- Nidhi Thesis PresentationDokument25 SeitenNidhi Thesis Presentationujjwal souravNoch keine Bewertungen
- Inguinal Hernia in Preterm Infants ( 32-Week Gestation) : Original ArticleDokument7 SeitenInguinal Hernia in Preterm Infants ( 32-Week Gestation) : Original ArticleBlank SpaceNoch keine Bewertungen
- Predictive factors for preeclampsiaDokument5 SeitenPredictive factors for preeclampsiaTiti Afrida SariNoch keine Bewertungen
- Oliverwilliams2015 PDFDokument10 SeitenOliverwilliams2015 PDFWh SquadNoch keine Bewertungen
- Maternal Complications Linked to Prolonged Second Stage LabourDokument9 SeitenMaternal Complications Linked to Prolonged Second Stage LabourwulanfarichahNoch keine Bewertungen
- Study of Management in Patient With Ectopic Pregnancy: Key WordsDokument3 SeitenStudy of Management in Patient With Ectopic Pregnancy: Key WordsparkfishyNoch keine Bewertungen
- NIH Public Access: Contributing Indications To The Rising Cesarean Delivery RateDokument17 SeitenNIH Public Access: Contributing Indications To The Rising Cesarean Delivery RatedianaNoch keine Bewertungen
- Pregnancy at Very Advanced Maternal Age: A UK Population-Based Cohort StudyDokument10 SeitenPregnancy at Very Advanced Maternal Age: A UK Population-Based Cohort StudyDM A27 RSU Haji SUBNoch keine Bewertungen
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyVon EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNoch keine Bewertungen
- Management of Hereditary Colorectal Cancer: A Multidisciplinary ApproachVon EverandManagement of Hereditary Colorectal Cancer: A Multidisciplinary ApproachJose G. GuillemNoch keine Bewertungen
- Current Concepts of Irritant Contact Dermatitis: J S C EnglishDokument6 SeitenCurrent Concepts of Irritant Contact Dermatitis: J S C EnglishMuhammad Riza FahlawiNoch keine Bewertungen
- Updated Treatment Prevention Migraine AdultDokument11 SeitenUpdated Treatment Prevention Migraine AdultMuhammad Riza FahlawiNoch keine Bewertungen
- Current Concepts of Irritant Contact Dermatitis: J S C EnglishDokument6 SeitenCurrent Concepts of Irritant Contact Dermatitis: J S C EnglishMuhammad Riza FahlawiNoch keine Bewertungen
- Irritant Contact Dermatitis: A Review: Professional Development ProgramDokument11 SeitenIrritant Contact Dermatitis: A Review: Professional Development ProgramMuhammad Riza FahlawiNoch keine Bewertungen
- Kocuria Dacryocystitis Infection, Caused by Kocuria Ocularis Sp. NovDokument4 SeitenKocuria Dacryocystitis Infection, Caused by Kocuria Ocularis Sp. NovMuhammad Riza FahlawiNoch keine Bewertungen
- Surat Lamaran CpnsDokument1 SeiteSurat Lamaran CpnsMuhammad Riza FahlawiNoch keine Bewertungen
- Updated Guideline UA, NSTEMI PDFDokument188 SeitenUpdated Guideline UA, NSTEMI PDFMuhammad Riza FahlawiNoch keine Bewertungen
- Bab 424 Terapi Non Farmakologi Pada DM PDFDokument4 SeitenBab 424 Terapi Non Farmakologi Pada DM PDFMuhammad Riza FahlawiNoch keine Bewertungen
- Kocuria Dacryocystitis Infection, Caused by Kocuria Ocularis Sp. NovDokument4 SeitenKocuria Dacryocystitis Infection, Caused by Kocuria Ocularis Sp. NovMuhammad Riza FahlawiNoch keine Bewertungen
- Acute dacryocystitis: another manifestation of sporotrichosisDokument3 SeitenAcute dacryocystitis: another manifestation of sporotrichosisMuhammad Riza FahlawiNoch keine Bewertungen
- A Systematic Review of Contact Dermatitis Treatment and PreventionDokument24 SeitenA Systematic Review of Contact Dermatitis Treatment and PreventionMuhammad Riza FahlawiNoch keine Bewertungen
- Kocuria Dacryocystitis Infection, Caused by Kocuria Ocularis Sp. NovDokument4 SeitenKocuria Dacryocystitis Infection, Caused by Kocuria Ocularis Sp. NovMuhammad Riza FahlawiNoch keine Bewertungen
- A Systematic Review of Contact Dermatitis Treatment and PreventionDokument24 SeitenA Systematic Review of Contact Dermatitis Treatment and PreventionMuhammad Riza FahlawiNoch keine Bewertungen
- Efficacy of Corticosteroids in Acute Experimental Irritant Contact Dermatitis?Dokument5 SeitenEfficacy of Corticosteroids in Acute Experimental Irritant Contact Dermatitis?Muhammad Riza FahlawiNoch keine Bewertungen
- Bab 427 Ketoasidosis Diabetik PDFDokument4 SeitenBab 427 Ketoasidosis Diabetik PDFMuhammad Riza FahlawiNoch keine Bewertungen
- Irritant Contact Dermatitis: A Review: Professional Development ProgramDokument11 SeitenIrritant Contact Dermatitis: A Review: Professional Development ProgramMuhammad Riza FahlawiNoch keine Bewertungen
- Bab 434 Neuropati Diabetik PDFDokument3 SeitenBab 434 Neuropati Diabetik PDFMuhammad Riza FahlawiNoch keine Bewertungen
- A Systematic Review of Contact Dermatitis Treatment and PreventionDokument24 SeitenA Systematic Review of Contact Dermatitis Treatment and PreventionMuhammad Riza FahlawiNoch keine Bewertungen
- Contact Dermatitis BJD Guidelines May 2009Dokument9 SeitenContact Dermatitis BJD Guidelines May 2009Cynthia OktariszaNoch keine Bewertungen
- Bab 422 Diagnosis Dan Klasifikasi Diabetes Melitus PDFDokument3 SeitenBab 422 Diagnosis Dan Klasifikasi Diabetes Melitus PDFMuhammad Riza FahlawiNoch keine Bewertungen
- Bab 428 Koma Hiperosmolar Hiperglikemik Non KetotikDokument3 SeitenBab 428 Koma Hiperosmolar Hiperglikemik Non KetotikLhandd'smartAlexander BbfplusmeofChibyNoch keine Bewertungen
- Bab 424 Terapi Non Farmakologi Pada DMDokument4 SeitenBab 424 Terapi Non Farmakologi Pada DMMuhammad Riza FahlawiNoch keine Bewertungen
- 1 SMDokument13 Seiten1 SMNia amaliaNoch keine Bewertungen
- PDFDokument130 SeitenPDFMuhammad Riza FahlawiNoch keine Bewertungen
- 0430130Dokument7 Seiten0430130Muhammad Riza FahlawiNoch keine Bewertungen
- 2090 2697 2 108 PDFDokument5 Seiten2090 2697 2 108 PDFMuhammad Riza FahlawiNoch keine Bewertungen
- Doxycyclin Alkaloid 100mg Capsules - ZIDokument12 SeitenDoxycyclin Alkaloid 100mg Capsules - ZIMaja TrajanovikjNoch keine Bewertungen
- PEDIA QUIZ CARDIORESPI and NEPHRODokument5 SeitenPEDIA QUIZ CARDIORESPI and NEPHROAlessa Mikkah BaltazarNoch keine Bewertungen
- Paediatric ART Initiation and Follow UpDokument33 SeitenPaediatric ART Initiation and Follow UpChetan AdsulNoch keine Bewertungen
- Anthelmintic Activity of Vidangadi Churna: Research ArticleDokument2 SeitenAnthelmintic Activity of Vidangadi Churna: Research ArticlegaurnityanandaNoch keine Bewertungen
- COVID-19 Prevention and Control Literature ReviewDokument2 SeitenCOVID-19 Prevention and Control Literature ReviewericNoch keine Bewertungen
- Clinical Characteristics of Raoultella Ornithinolytica BacteremiaDokument6 SeitenClinical Characteristics of Raoultella Ornithinolytica BacteremiaEnrique MartínezNoch keine Bewertungen
- Doc. AP Bio FRQ Biotech KEY PDFDokument11 SeitenDoc. AP Bio FRQ Biotech KEY PDFMichael JuniorNoch keine Bewertungen
- Literature Review Acute GastroenteritisDokument8 SeitenLiterature Review Acute Gastroenteritisc5hzgcdj100% (1)
- Needle Prick InjuryDokument20 SeitenNeedle Prick InjuryThirugnanaThiruNoch keine Bewertungen
- Fungal and Viral ReplicationDokument22 SeitenFungal and Viral ReplicationAbigail Mayled LausNoch keine Bewertungen
- Biological HazaDokument3 SeitenBiological HazaVladimere Censon ReyesNoch keine Bewertungen
- ThlasmiaDokument7 SeitenThlasmiaSonia AhmedNoch keine Bewertungen
- Infectious Mononucleosis: Clinical PracticeDokument8 SeitenInfectious Mononucleosis: Clinical PracticeSamara Motter DetoniNoch keine Bewertungen
- Best Insight Specialty-Paeds TeamDokument56 SeitenBest Insight Specialty-Paeds TeamSaQlain BalochNoch keine Bewertungen
- Chapter Overview: 8: FungiDokument17 SeitenChapter Overview: 8: FungiBianca ElbrechtNoch keine Bewertungen
- Dengue Fever /dengue Hemorrhagic Fever: Dr. Harun Hudari, SPPD FinasimDokument66 SeitenDengue Fever /dengue Hemorrhagic Fever: Dr. Harun Hudari, SPPD Finasimekafebri88Noch keine Bewertungen
- Managing Pain After AppendectomyDokument2 SeitenManaging Pain After AppendectomyChatoh SanaoNoch keine Bewertungen
- Goldman Report-Corona Impact PDFDokument25 SeitenGoldman Report-Corona Impact PDFsumitbajaj100% (1)
- 12 ISC Biology 1 - 230518 - 161521Dokument10 Seiten12 ISC Biology 1 - 230518 - 161521Parth GuptaNoch keine Bewertungen
- Daily IDSP Report On 29.07.2017Dokument14 SeitenDaily IDSP Report On 29.07.2017Anonymous woB6M9Noch keine Bewertungen
- K6 - Tetanus PEDIATRICDokument23 SeitenK6 - Tetanus PEDIATRICbanuperiahNoch keine Bewertungen
- Anti-Protozoal Drugs FinalizedDokument54 SeitenAnti-Protozoal Drugs FinalizedMoazama Fayyaz100% (1)
- Asperheim/Favaro: Introduction To Pharmacology, 12th EditionDokument2 SeitenAsperheim/Favaro: Introduction To Pharmacology, 12th Editionvinhson65-1Noch keine Bewertungen
- ReferencesDokument94 SeitenReferencesElise SwaelesNoch keine Bewertungen