Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- Ehx 419Dokument48 SeitenEhx 419Adriana VasilicaNoch keine Bewertungen
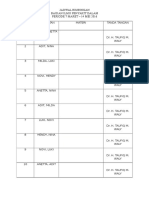
- Jadwal Bimbingan Bagian Ilmu Penyakit Dalam Periode 7 Maret - 14 Mei 2016Dokument1 SeiteJadwal Bimbingan Bagian Ilmu Penyakit Dalam Periode 7 Maret - 14 Mei 2016tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- Anemia 2013Dokument19 SeitenAnemia 2013tio_bsNoch keine Bewertungen
- 4Dokument1 Seite4tio_bsNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 15-Statutory Report Statutory Define Law (Legal Protection) Statutory MeetingDokument2 Seiten15-Statutory Report Statutory Define Law (Legal Protection) Statutory MeetingRaima DollNoch keine Bewertungen
- Water Security STD 9th Textbook by Techy BagDokument86 SeitenWater Security STD 9th Textbook by Techy Bagpooja TiwariNoch keine Bewertungen
- A Walk in The Physical - Christian SundbergDokument282 SeitenA Walk in The Physical - Christian SundbergKatie MhNoch keine Bewertungen
- Report On Marketing of ArecanutDokument22 SeitenReport On Marketing of ArecanutsivakkmNoch keine Bewertungen
- Reading Test - 3 Clinical Depression Text ADokument17 SeitenReading Test - 3 Clinical Depression Text AJisha JanardhanNoch keine Bewertungen
- Phyilosophy of Midwifery Care 2Dokument13 SeitenPhyilosophy of Midwifery Care 2Noella BezzinaNoch keine Bewertungen
- הרצאה- אנמיה וטרומבוציטופניהDokument87 Seitenהרצאה- אנמיה וטרומבוציטופניהliatfurmanNoch keine Bewertungen
- All India Quota Medical Seats (MBBS) With AIPMT 2015 Score PDFDokument5 SeitenAll India Quota Medical Seats (MBBS) With AIPMT 2015 Score PDFjuhiNoch keine Bewertungen
- Gulayan Sa Barangay OrdinanceDokument2 SeitenGulayan Sa Barangay OrdinancekonsinoyeNoch keine Bewertungen
- ICT ContactCenterServices 9 Q1 LAS3 FINALDokument10 SeitenICT ContactCenterServices 9 Q1 LAS3 FINALRomnia Grace DivinagraciaNoch keine Bewertungen
- PLAB 2 VISA Guidelines by Omar AlamDokument18 SeitenPLAB 2 VISA Guidelines by Omar Alamrafew19Noch keine Bewertungen
- All Vaccinees Are Requested To Bring Certificate of Dose-II From COWIN Portal Alongwith Registered Mobile Number Before Proceeding For VaccinationDokument7 SeitenAll Vaccinees Are Requested To Bring Certificate of Dose-II From COWIN Portal Alongwith Registered Mobile Number Before Proceeding For VaccinationRakesh KumarNoch keine Bewertungen
- Information Technology Solutions: ADMET Testing SystemsDokument2 SeitenInformation Technology Solutions: ADMET Testing Systemskrishgen biosystemsNoch keine Bewertungen
- Thornburg Letter of RecDokument1 SeiteThornburg Letter of Recapi-511764033Noch keine Bewertungen
- Ulangan Tengah Semester: Mata Pelajaran Kelas: Bahasa Inggris: X Ak 1 / X Ak 2 Hari/ Tanggal: Waktu: 50 MenitDokument4 SeitenUlangan Tengah Semester: Mata Pelajaran Kelas: Bahasa Inggris: X Ak 1 / X Ak 2 Hari/ Tanggal: Waktu: 50 Menitmirah yuliarsianitaNoch keine Bewertungen
- Business-Plan (John Lloyd A Perido Grade 12-Arc)Dokument4 SeitenBusiness-Plan (John Lloyd A Perido Grade 12-Arc)Jaypher PeridoNoch keine Bewertungen
- Adjectives Comparative and Superlative FormDokument5 SeitenAdjectives Comparative and Superlative FormOrlando MiguelNoch keine Bewertungen
- Cooking VocabularyDokument2 SeitenCooking VocabularyDANIELANoch keine Bewertungen
- 56.vocal Warmup Log For Belt Your FaceDokument5 Seiten56.vocal Warmup Log For Belt Your FaceAlinutza AlinaNoch keine Bewertungen
- The Nursing ShortageDokument6 SeitenThe Nursing Shortageapi-455495817Noch keine Bewertungen
- Applying Sarf Book 1 - Published-46-59Dokument14 SeitenApplying Sarf Book 1 - Published-46-59Nauman AbbasNoch keine Bewertungen
- AudiometerDokument3 SeitenAudiometerVasanth VasanthNoch keine Bewertungen
- Schengen Certificate ExampleDokument2 SeitenSchengen Certificate ExampleGabriel Republi CanoNoch keine Bewertungen
- Child-Centered and Progressive EducationDokument2 SeitenChild-Centered and Progressive EducationDibyendu ChoudhuryNoch keine Bewertungen
- EV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoDokument2 SeitenEV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoCarolinaNoch keine Bewertungen
- Stats Review CH 1-6Dokument15 SeitenStats Review CH 1-6Megha BanerjeeNoch keine Bewertungen
- WB Food Processing IndustryDokument13 SeitenWB Food Processing IndustryRakesh KumarNoch keine Bewertungen
- Task 2: Health Services Survey: School Community 1. What Are The Health Services Provided?Dokument1 SeiteTask 2: Health Services Survey: School Community 1. What Are The Health Services Provided?Bernadeth BaiganNoch keine Bewertungen
- Chuyên Anh S Hà N I 2021Dokument5 SeitenChuyên Anh S Hà N I 2021Jennifer WatsonNoch keine Bewertungen