Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Effects of Preterm Birth On Oral Growth and Development: W. Kim Seow, MDSC, DDSC, PHD, FracdsDokument7 SeitenEffects of Preterm Birth On Oral Growth and Development: W. Kim Seow, MDSC, DDSC, PHD, FracdsBanyu علي تقويم BiruNoch keine Bewertungen
- Paulsson2019 Article TheImpactOfPrematureBirthOnDenDokument7 SeitenPaulsson2019 Article TheImpactOfPrematureBirthOnDenBanyu علي تقويم BiruNoch keine Bewertungen
- Avulsion and Replantation of Primary Teeth A Feasible OptionDokument3 SeitenAvulsion and Replantation of Primary Teeth A Feasible OptionSushmita AlmiraNoch keine Bewertungen
- The Superior Labial Frenulum in Newborns: What Is Normal?Dokument6 SeitenThe Superior Labial Frenulum in Newborns: What Is Normal?Banyu علي تقويم BiruNoch keine Bewertungen
- (Balkan Journal of Dental Medicine) Prosthetics in Paediatric DentistryDokument5 Seiten(Balkan Journal of Dental Medicine) Prosthetics in Paediatric DentistryShreya DasguptaNoch keine Bewertungen
- Dental Health in Children Born Very Preterm.: Neonatal, Paediatric and Child Health Nursing January 2004Dokument4 SeitenDental Health in Children Born Very Preterm.: Neonatal, Paediatric and Child Health Nursing January 2004Banyu علي تقويم BiruNoch keine Bewertungen
- Prevalence of Dental Caries and Caries-Related Risk Factors in Premature and Term ChildrenDokument7 SeitenPrevalence of Dental Caries and Caries-Related Risk Factors in Premature and Term ChildrenBanyu علي تقويم BiruNoch keine Bewertungen
- Pesquisa Brasileira em Odontopediatria e Clínica Integrada 1519-0501Dokument13 SeitenPesquisa Brasileira em Odontopediatria e Clínica Integrada 1519-0501Banyu علي تقويم BiruNoch keine Bewertungen
- A Review of The Eruption of Primary Teeth: Chchu, C Y YeungDokument6 SeitenA Review of The Eruption of Primary Teeth: Chchu, C Y YeungBanyu علي تقويم BiruNoch keine Bewertungen
- Pesquisa Brasileira em Odontopediatria e Clínica Integrada 1519-0501Dokument13 SeitenPesquisa Brasileira em Odontopediatria e Clínica Integrada 1519-0501Banyu علي تقويم BiruNoch keine Bewertungen
- Brunilda Dhamo PHD ThesisDokument200 SeitenBrunilda Dhamo PHD ThesisBanyu علي تقويم BiruNoch keine Bewertungen
- Maternal and Early Life Factors of Tooth Emergence PatternsDokument26 SeitenMaternal and Early Life Factors of Tooth Emergence PatternsBanyu علي تقويم BiruNoch keine Bewertungen
- Dental Caries in Thalassemia Patients at SrinagariDokument6 SeitenDental Caries in Thalassemia Patients at SrinagariBanyu علي تقويم BiruNoch keine Bewertungen
- Effects of Green Tea On Periodontal Health: A Prospective Clinical StudyDokument7 SeitenEffects of Green Tea On Periodontal Health: A Prospective Clinical StudyBanyu علي تقويم BiruNoch keine Bewertungen
- The Effect of Breast Feeding On Eruption of First Primary Tooth in A Group of 6-12 Month Saudi ChildrenDokument6 SeitenThe Effect of Breast Feeding On Eruption of First Primary Tooth in A Group of 6-12 Month Saudi ChildrenBanyu علي تقويم BiruNoch keine Bewertungen
- Tooth Eruption Disorders Associated With Systemic and Genetic Diseases: Clinical GuideDokument16 SeitenTooth Eruption Disorders Associated With Systemic and Genetic Diseases: Clinical GuideBanyu علي تقويم BiruNoch keine Bewertungen
- Effect of Developmental Milestones On Patterns of Teeth EruptionDokument4 SeitenEffect of Developmental Milestones On Patterns of Teeth EruptionBanyu علي تقويم BiruNoch keine Bewertungen
- Piis1875957210600447 PDFDokument3 SeitenPiis1875957210600447 PDFBanyu علي تقويم BiruNoch keine Bewertungen
- Science Behind Human SalivaDokument6 SeitenScience Behind Human SalivaBanyu علي تقويم BiruNoch keine Bewertungen
- G Infantoralhealthcare PDFDokument5 SeitenG Infantoralhealthcare PDFBanyu علي تقويم BiruNoch keine Bewertungen
- Folayan2010 Article BreastfeedingTimingAndNumberOfDokument4 SeitenFolayan2010 Article BreastfeedingTimingAndNumberOfBanyu علي تقويم BiruNoch keine Bewertungen
- OralHealthFCpagesF2 2 1Dokument18 SeitenOralHealthFCpagesF2 2 1Banyu علي تقويم BiruNoch keine Bewertungen
- JurnalDokument5 SeitenJurnalBanyu علي تقويم BiruNoch keine Bewertungen
- IndianJOralSci3294-3184465 085044Dokument5 SeitenIndianJOralSci3294-3184465 085044Banyu علي تقويم BiruNoch keine Bewertungen
- Daftar PustakaDokument5 SeitenDaftar PustakaBanyu علي تقويم BiruNoch keine Bewertungen
- Mock Up in DentistryDokument15 SeitenMock Up in DentistryBanyu علي تقويم BiruNoch keine Bewertungen
- Tagline International Babywearers Week 2017Dokument3 SeitenTagline International Babywearers Week 2017Banyu علي تقويم BiruNoch keine Bewertungen
- G Restorative PDFDokument12 SeitenG Restorative PDFerma gusmayantiNoch keine Bewertungen
- Surat RiskesdasDokument2 SeitenSurat RiskesdasBanyu علي تقويم BiruNoch keine Bewertungen
- Menu Word Problems Worksheet #4: NameDokument2 SeitenMenu Word Problems Worksheet #4: NameKoushiik KumarNoch keine Bewertungen
- Management of The Sick Young Infant Aged Up To 2 Month (Long)Dokument1 SeiteManagement of The Sick Young Infant Aged Up To 2 Month (Long)Jsper TbyanNoch keine Bewertungen
- Sudoku Playoffs CBDokument8 SeitenSudoku Playoffs CBDi CatNoch keine Bewertungen
- 2e. AAP Tongue Tie FrenotomyDokument2 Seiten2e. AAP Tongue Tie FrenotomyAprilian Ayu SitaNoch keine Bewertungen
- Breastfeeding and The Fascial System.Dokument3 SeitenBreastfeeding and The Fascial System.jenniferspak100% (2)
- Bonding With Baby in The Early DaysDokument3 SeitenBonding With Baby in The Early DaysAnnisatus SholehahNoch keine Bewertungen
- Giving Birth To TwinsDokument2 SeitenGiving Birth To Twinsadw_coolNoch keine Bewertungen
- Factors That Influence Postpartum RecoveryDokument2 SeitenFactors That Influence Postpartum RecoveryHelenice Assis VespasianoNoch keine Bewertungen
- Paed History TakingDokument2 SeitenPaed History TakingWong Lee ThengNoch keine Bewertungen
- Jose James LyricsDokument7 SeitenJose James LyricsMilan KocićNoch keine Bewertungen
- 9 Month Asq3 2Dokument10 Seiten9 Month Asq3 2api-377093974Noch keine Bewertungen
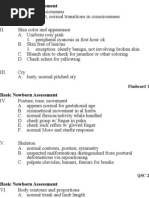
- Basic Newborn Assessment FlashcardsDokument7 SeitenBasic Newborn Assessment FlashcardsChristina Chaston MonteithNoch keine Bewertungen
- 68 Pacifier (Dokument3 Seiten68 Pacifier (Gokull ShautriNoch keine Bewertungen
- Face Breech BrowDokument4 SeitenFace Breech BrowIsaiah AmolatoNoch keine Bewertungen
- Birthday Magic SquareDokument19 SeitenBirthday Magic SquareAmarnath Murthy50% (4)
- Baby Tips For MumsDokument98 SeitenBaby Tips For MumsGiao Con100% (1)
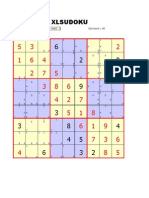
- XL SudokuDokument15 SeitenXL SudokuruytguerraNoch keine Bewertungen
- Essential Newborn Care ProtocolDokument30 SeitenEssential Newborn Care ProtocolGwendareign ElizanNoch keine Bewertungen
- SleepDokument29 SeitenSleepjosephnavyNoch keine Bewertungen
- LAPTARE Copii Cu Patologie...Dokument8 SeitenLAPTARE Copii Cu Patologie...Claudia KosztelnikNoch keine Bewertungen
- Tongue Tie AAPD 2004 Classification, TreatmentDokument7 SeitenTongue Tie AAPD 2004 Classification, TreatmentDilmohit SinghNoch keine Bewertungen
- Sesi 6-How Milk Gets From Breast To BabyDokument32 SeitenSesi 6-How Milk Gets From Breast To BabyMazlina Maidin100% (1)
- Mini - Course On Temperature Control in The Newborn: InstructionsDokument21 SeitenMini - Course On Temperature Control in The Newborn: InstructionsAbu RaiahanNoch keine Bewertungen