Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Atmakaraka PDFDokument46 SeitenAtmakaraka PDFrohitsingh_8150% (4)
- E2309 137950-1Dokument8 SeitenE2309 137950-1Sarvesh MishraNoch keine Bewertungen
- Windows XP Short KeysDokument4 SeitenWindows XP Short KeysmaheshrvrNoch keine Bewertungen
- Chords Lyrics ColbieDokument4 SeitenChords Lyrics ColbiecarmaxetaNoch keine Bewertungen
- Ideal NCPDokument2 SeitenIdeal NCPcarmaxetaNoch keine Bewertungen
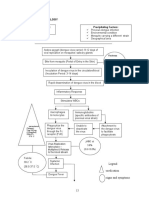
- Pathophysiology of Our Case Study Viral Myocarditis Secondary To Dengue FeverDokument2 SeitenPathophysiology of Our Case Study Viral Myocarditis Secondary To Dengue FevercarmaxetaNoch keine Bewertungen
- Influenza Nausea and Vomiting FeverDokument20 SeitenInfluenza Nausea and Vomiting FevercarmaxetaNoch keine Bewertungen
- Actual NCPDokument3 SeitenActual NCPcarmaxeta100% (2)
- Drug StudyDokument5 SeitenDrug StudycarmaxetaNoch keine Bewertungen
- Actual NCPDokument3 SeitenActual NCPcarmaxeta100% (2)
- Bancroftian FilariasisDokument6 SeitenBancroftian FilariasiscarmaxetaNoch keine Bewertungen
- Clinical Mental Health Counseling in Community and Agency Settings 5Th Edition Full ChapterDokument41 SeitenClinical Mental Health Counseling in Community and Agency Settings 5Th Edition Full Chapterwilliam.kellar832100% (24)
- Practical Kabbalah: Jewish Mysticism, Meditation and MoralityDokument4 SeitenPractical Kabbalah: Jewish Mysticism, Meditation and MoralityJoyce Choombe MulengaNoch keine Bewertungen
- Climate and Urban FormDokument10 SeitenClimate and Urban FormYunita RatihNoch keine Bewertungen
- Reflection Paper - InternshipDokument7 SeitenReflection Paper - Internshipapi-549362324Noch keine Bewertungen
- Lesson 3 Christianity ModuleDokument20 SeitenLesson 3 Christianity ModuleCharmaine Alexi PaclibarNoch keine Bewertungen
- Activities For Phonemic AwarenessDokument4 SeitenActivities For Phonemic AwarenessSpriha Agarwal100% (1)
- 7 Basic Control ActionsDokument27 Seiten7 Basic Control ActionsAhmad ElsheemyNoch keine Bewertungen
- TQM 2 MARKSDokument12 SeitenTQM 2 MARKSMARIYAPPANNoch keine Bewertungen
- ĐỀ CHUẨN MINH HỌA SỐ 03Dokument17 SeitenĐỀ CHUẨN MINH HỌA SỐ 03Lê Thị Ngọc ÁnhNoch keine Bewertungen
- An ISO 9001Dokument3 SeitenAn ISO 9001Prasad IngoleNoch keine Bewertungen
- RepigmentationDokument4 SeitenRepigmentationMariyaNoch keine Bewertungen
- Analysis and Design of Circular Beams-2017Dokument49 SeitenAnalysis and Design of Circular Beams-2017Ragheb Ibrahim0% (1)
- SSC 146G Summer 2016 Human Sexuality SyllabusDokument1 SeiteSSC 146G Summer 2016 Human Sexuality SyllabusJames SmithNoch keine Bewertungen
- Void For Vagueness DoctrineDokument16 SeitenVoid For Vagueness Doctrinefatima ramosNoch keine Bewertungen
- Schools of PsychologyDokument30 SeitenSchools of PsychologyMdl C DayritNoch keine Bewertungen
- Book Review: Alain de Botton's The Art of TravelDokument8 SeitenBook Review: Alain de Botton's The Art of TravelharroweenNoch keine Bewertungen
- Enuma Elish LitChartDokument20 SeitenEnuma Elish LitChartsugarntea24Noch keine Bewertungen
- Assessment - The Bridge Between Teaching and Learning (VFTM 2013)Dokument6 SeitenAssessment - The Bridge Between Teaching and Learning (VFTM 2013)Luis CYNoch keine Bewertungen
- Unit 8Dokument2 SeitenUnit 8The Four QueensNoch keine Bewertungen
- MRI BRAIN FINAL DR Shamol PDFDokument306 SeitenMRI BRAIN FINAL DR Shamol PDFDrSunil Kumar DasNoch keine Bewertungen
- Urology Case Reports: Shakhawan Hama Amin Said, Rezhin Yaseen Abdalla, Ismaeel Aghaways, Ari Mohammed AbdullahDokument3 SeitenUrology Case Reports: Shakhawan Hama Amin Said, Rezhin Yaseen Abdalla, Ismaeel Aghaways, Ari Mohammed AbdullahHardiTariqHammaNoch keine Bewertungen
- (13-14) - Modeling of Thermal SystemsDokument33 Seiten(13-14) - Modeling of Thermal SystemsmawooaNoch keine Bewertungen
- Belief MatrixDokument1 SeiteBelief Matrixapi-384108912Noch keine Bewertungen
- ManipalCigna Active Retail Hospital Network List as on 01 Apr 2022Dokument415 SeitenManipalCigna Active Retail Hospital Network List as on 01 Apr 2022sanjay kumarNoch keine Bewertungen
- TO B.inggris Dzakiy Bag 2Dokument21 SeitenTO B.inggris Dzakiy Bag 2Ayu RatnaNoch keine Bewertungen
- Bolomeya Model For Normal Concrete Mix DesignDokument6 SeitenBolomeya Model For Normal Concrete Mix DesignprincessrandotaNoch keine Bewertungen
- Peta I Think Fizik t4Dokument18 SeitenPeta I Think Fizik t4Yk TayNoch keine Bewertungen
- Planning Worksheet For Access and QualityDokument3 SeitenPlanning Worksheet For Access and QualityBar BetsNoch keine Bewertungen