Das könnte Ihnen auch gefallen
- 634709499523281250Dokument34 Seiten634709499523281250BINDUNoch keine Bewertungen
- 634150422011571250Dokument33 Seiten634150422011571250BINDU0% (1)
- Selectivity Electrophysiology Continued: V-Gating The Speed of Spike Propagation and The Geometry of The Axon Role of MyelinationDokument34 SeitenSelectivity Electrophysiology Continued: V-Gating The Speed of Spike Propagation and The Geometry of The Axon Role of MyelinationBINDUNoch keine Bewertungen
- K Channels: Biochemistry of MetabolismDokument23 SeitenK Channels: Biochemistry of MetabolismBINDUNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- BPR Guidance Ra Vol IV Part B-C enDokument416 SeitenBPR Guidance Ra Vol IV Part B-C enPepe Jara GinsbergNoch keine Bewertungen
- PP No.74 TH 2001 Lampiran II PDFDokument5 SeitenPP No.74 TH 2001 Lampiran II PDFFita Mei suryaningsihNoch keine Bewertungen
- Pharmaceutical Toxicology Manual FINALDokument76 SeitenPharmaceutical Toxicology Manual FINALmasorNoch keine Bewertungen
- The Best - Deadly Poisons, Ingested or InhaledDokument1 SeiteThe Best - Deadly Poisons, Ingested or InhaledSyncOrSwim100% (1)
- Powerpoint Module 3 PDFDokument28 SeitenPowerpoint Module 3 PDFnaveed ahmedNoch keine Bewertungen
- Jurnal PenelitianDokument12 SeitenJurnal PenelitianYanto FransiscusNoch keine Bewertungen
- Toxicology Problem Set WordDokument7 SeitenToxicology Problem Set Wordapi-235658421Noch keine Bewertungen
- Pool of Research ScholarDokument404 SeitenPool of Research ScholarN Inbasagaran100% (1)
- Report On Carcinogens 13th Edition The 508Dokument2 SeitenReport On Carcinogens 13th Edition The 508SaiKai54Noch keine Bewertungen
- Green Chilli ReportDokument3 SeitenGreen Chilli ReportPankaj GaikwadNoch keine Bewertungen
- Dasar ToksikologiDokument47 SeitenDasar ToksikologiAmirul Rahmat AlfaisalNoch keine Bewertungen
- 6 - Environmental Health PDFDokument8 Seiten6 - Environmental Health PDFAbo AmgadNoch keine Bewertungen
- FDA Guidance For Industry S7a Safety Pharmacology Studies For Human Pharmaceuticals PDFDokument14 SeitenFDA Guidance For Industry S7a Safety Pharmacology Studies For Human Pharmaceuticals PDFbmartindoyle6396Noch keine Bewertungen
- T o X I C o L o G yDokument7 SeitenT o X I C o L o G yDennis ValdezNoch keine Bewertungen
- Iso 10993 1 2018 en PDFDokument11 SeitenIso 10993 1 2018 en PDFPhạm Thu HuyềnNoch keine Bewertungen
- Jenke 2017Dokument10 SeitenJenke 2017cute babyNoch keine Bewertungen
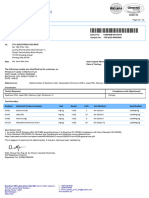
- Stretch Film RoHS Test ReportDokument2 SeitenStretch Film RoHS Test ReportAmirun AeimanzzNoch keine Bewertungen
- Forensics ManualDokument227 SeitenForensics ManualWilfredo P. Sudio, Jr.Noch keine Bewertungen
- Banned and Category 1 Pesticides and Herbicides That Have Been Used in Aquaculture or Found in Aquaculture ProductsDokument22 SeitenBanned and Category 1 Pesticides and Herbicides That Have Been Used in Aquaculture or Found in Aquaculture ProductsHejie QiuNoch keine Bewertungen
- Developmental Endocrine Reproductive Toxicologist in NJ NY Resume Edward FrizellDokument7 SeitenDevelopmental Endocrine Reproductive Toxicologist in NJ NY Resume Edward FrizellEdwardFrizellNoch keine Bewertungen
- Green Solvents For Chemistry - Perspectives and Practice - W. Nelson (Oxford, 2003) WW PDFDokument399 SeitenGreen Solvents For Chemistry - Perspectives and Practice - W. Nelson (Oxford, 2003) WW PDFapc108Noch keine Bewertungen
- Drilling Mud Base FluidDokument2 SeitenDrilling Mud Base FluidderekfisherNoch keine Bewertungen
- MSDS-Redispersible Polymer PowderDokument10 SeitenMSDS-Redispersible Polymer PowderFátima Julieta García AguilarNoch keine Bewertungen
- Gerald: Dental Fillings / Mercury Poisoning / UCSF School of Medicine-Winter 1989Dokument55 SeitenGerald: Dental Fillings / Mercury Poisoning / UCSF School of Medicine-Winter 1989Gerald Russell100% (1)
- Joint Action of InsecticidesDokument31 SeitenJoint Action of Insecticidessyed100% (2)
- GuidelineeuropamicrobiologiaDokument106 SeitenGuidelineeuropamicrobiologiakeinthfNoch keine Bewertungen
- MedicineComplete CLARK DRUG AND POISONDokument25 SeitenMedicineComplete CLARK DRUG AND POISONBarca StanNoch keine Bewertungen
- Poisons ActDokument12 SeitenPoisons ActPatel sunitaNoch keine Bewertungen
- Agad Tantra CME Revised ModuleDokument15 SeitenAgad Tantra CME Revised ModuleDr. Nishant BarapatreNoch keine Bewertungen
- E BooksDokument29 SeitenE BooksTawfeeq BA Abbad100% (2)