Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Pharmacy-Immunology 19: Primary & Acquired Immunodeficiency Saber HusseinDokument18 SeitenPharmacy-Immunology 19: Primary & Acquired Immunodeficiency Saber Husseinmmoney1Noch keine Bewertungen
- Vaccinated Vs Unvaccinated Homeschooled Kids Can You Guess Who Is HealthierDokument5 SeitenVaccinated Vs Unvaccinated Homeschooled Kids Can You Guess Who Is Healthier300rNoch keine Bewertungen
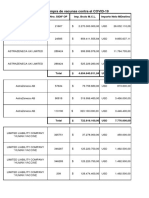
- Pagos Efectuados A LaboratoriosDokument14 SeitenPagos Efectuados A LaboratoriosCronista.comNoch keine Bewertungen
- Microbiology Burton's Chapter 16Dokument74 SeitenMicrobiology Burton's Chapter 16Whenzhie Villaverde PampoNoch keine Bewertungen
- ADA en TBCDokument6 SeitenADA en TBCNorma Ruth Aguilar CarbajalNoch keine Bewertungen
- Idiopathic Inflammatory MyopathyDokument24 SeitenIdiopathic Inflammatory MyopathyAgeededin HartNoch keine Bewertungen
- Spleen Histology and Hematology of Mice after E. coli Infection and Humic Acid AdministrationDokument9 SeitenSpleen Histology and Hematology of Mice after E. coli Infection and Humic Acid AdministrationMyusik ZNoch keine Bewertungen
- BB Lab MidtermDokument3 SeitenBB Lab MidtermYo Issei HyodonoNoch keine Bewertungen
- Reducing Malaria Infections in Sub-Saharan AfricaDokument2 SeitenReducing Malaria Infections in Sub-Saharan AfricaStansa SeniaNoch keine Bewertungen
- Chronic Urticaria Clinical Presentation - History, Physical Examination, ComplicationsDokument5 SeitenChronic Urticaria Clinical Presentation - History, Physical Examination, ComplicationsOgy SkillNoch keine Bewertungen
- Tissue Nematodes ClassificationDokument33 SeitenTissue Nematodes ClassificationJessiNoch keine Bewertungen
- Lower Genital Infections GuideDokument2 SeitenLower Genital Infections Guidecbac1990Noch keine Bewertungen
- Urticaria and Angioedema: Ailing Zou (邹爱玲) 2021.10.18Dokument24 SeitenUrticaria and Angioedema: Ailing Zou (邹爱玲) 2021.10.18AmeliaNoch keine Bewertungen
- IB Biology Topic 11 - Animal Physiology HL Revision SheetDokument1 SeiteIB Biology Topic 11 - Animal Physiology HL Revision SheetLexieNoch keine Bewertungen
- Ebook - Understanding Immune Cell Function in Cancer - IsoPlexisDokument7 SeitenEbook - Understanding Immune Cell Function in Cancer - IsoPlexisJ VelazcoNoch keine Bewertungen
- Poststreptococcal Glomerulonephritis - UpToDateDokument21 SeitenPoststreptococcal Glomerulonephritis - UpToDateHandre Putra100% (1)
- Rounds: Case Study and Review of Autoimmune HepatitisDokument7 SeitenRounds: Case Study and Review of Autoimmune HepatitisClaudia Naomi Ventura OrtizNoch keine Bewertungen
- PP Insect Bite 2007Dokument16 SeitenPP Insect Bite 2007Ali RumiNoch keine Bewertungen
- Raw 2 LawsDokument17 SeitenRaw 2 LawsRed HaleNoch keine Bewertungen
- Actinomycosis, Tuberculosis, Leprosy, Syphilis, NomaDokument37 SeitenActinomycosis, Tuberculosis, Leprosy, Syphilis, NomaAroosha MasoodNoch keine Bewertungen
- Hematology 1Dokument4 SeitenHematology 1Ayra Celine Gem ManabatNoch keine Bewertungen
- Anti CCP TestDokument3 SeitenAnti CCP TestDr ANAS MUNSHINoch keine Bewertungen
- Blood Tranfusion 2016 PPNIDokument60 SeitenBlood Tranfusion 2016 PPNIMartin HermawanNoch keine Bewertungen
- Chapter 8..... HypersensitivityDokument6 SeitenChapter 8..... HypersensitivityShama AftabNoch keine Bewertungen
- Ag Ab ReactionsDokument43 SeitenAg Ab ReactionsNiyaz ShahriarNoch keine Bewertungen
- Geographic Identifiers CHNNDokument3 SeitenGeographic Identifiers CHNNjaira magbanuaNoch keine Bewertungen
- Format Pendataan Posyandu Sasaran Bian PKM Pondok Gede JatiwaringinDokument407 SeitenFormat Pendataan Posyandu Sasaran Bian PKM Pondok Gede JatiwaringinparamitaNoch keine Bewertungen
- Opportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaDokument4 SeitenOpportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaPinay YaunNoch keine Bewertungen
- COVID-19 consumable products catalogDokument2 SeitenCOVID-19 consumable products catalogRadit AMSNoch keine Bewertungen
- Pathogenic BacteriaDokument6 SeitenPathogenic BacteriaNit ZeNoch keine Bewertungen