Das könnte Ihnen auch gefallen
- Antidepressant Comparison ChartDokument3 SeitenAntidepressant Comparison Chartiggyputtty100% (29)
- Psychotropic Drugs.Dokument15 SeitenPsychotropic Drugs.Xiaoqing SongNoch keine Bewertungen
- Antidepressant ChartDokument7 SeitenAntidepressant Chartinher1tance100% (4)
- Psychopharmacology 2 AntidepressantsDokument7 SeitenPsychopharmacology 2 AntidepressantsBea Samonte100% (2)
- Common Psychiatric TermsDokument6 SeitenCommon Psychiatric TermsKatrina Heart Rauto AvilaNoch keine Bewertungen
- "Serotonin Syndrome Causes HARM": Psychiatry PharamacologyDokument9 Seiten"Serotonin Syndrome Causes HARM": Psychiatry Pharamacologytycobb63100% (4)
- Depression in Older Adults: A Treatable Medical ConditionDokument12 SeitenDepression in Older Adults: A Treatable Medical ConditionJose Alonso Aguilar Valera100% (1)
- AntidepressantsDokument5 SeitenAntidepressantsUm HamoOd100% (2)
- Psychiatry textbook and reference guide collectionDokument4 SeitenPsychiatry textbook and reference guide collectionIbrahimFikryNoch keine Bewertungen
- Antipsychotic DrugsDokument47 SeitenAntipsychotic DrugsIkram UddinNoch keine Bewertungen
- The PSYCH MAP ColoredDokument2 SeitenThe PSYCH MAP Coloredcentrino17Noch keine Bewertungen
- Psychiatry - Shelf ReviewDokument101 SeitenPsychiatry - Shelf Reviewluck2liv100% (4)
- Handbook of Psychiatric DrugsDokument68 SeitenHandbook of Psychiatric Drugsbson100% (13)
- Handy Summary Chart Comparing The Main Medications For DepressionDokument2 SeitenHandy Summary Chart Comparing The Main Medications For Depressionrowanpurdy100% (4)
- Psychiatry: AntidepressantsDokument2 SeitenPsychiatry: AntidepressantsSok-Moi Chok100% (1)
- Psychiatry: Mental State ExaminationDokument3 SeitenPsychiatry: Mental State ExaminationSok-Moi Chok100% (3)
- Drug List Psych Optho NeuroDokument22 SeitenDrug List Psych Optho NeuroAshley BarrileNoch keine Bewertungen
- ANTIPSYCHOTICSDokument25 SeitenANTIPSYCHOTICSCheetahboi Shopee100% (4)
- Psychiatry MnemonicsDokument4 SeitenPsychiatry MnemonicsHiruni Tharuka100% (2)
- Reviewer On PsychopharmacologyDokument28 SeitenReviewer On PsychopharmacologyKristine Ann Hernandez100% (1)
- PsychopharmacologyDokument64 SeitenPsychopharmacologyGaurav Tandon100% (2)
- Glossary of Psychiatric TermsDokument42 SeitenGlossary of Psychiatric TermsÏtz ShãrîNoch keine Bewertungen
- AntipsychoticsDokument51 SeitenAntipsychoticsShailja SharmaNoch keine Bewertungen
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDokument6 SeitenAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNoch keine Bewertungen
- Sudden Onset (Within 2 Weeks) of at Least One of TheDokument2 SeitenSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNoch keine Bewertungen
- Mood Disorders: Depressive Disorders: Bipolar DisordersDokument4 SeitenMood Disorders: Depressive Disorders: Bipolar DisordersWen Jie LauNoch keine Bewertungen
- Treatment Modalities For Mood DisordersDokument55 SeitenTreatment Modalities For Mood DisordersGlory MimiNoch keine Bewertungen
- Pharmacotherapy in PschiatryDokument8 SeitenPharmacotherapy in PschiatryygfhdgNoch keine Bewertungen
- Antipsychotics Guide for Nursing Intervention and Patient EducationDokument10 SeitenAntipsychotics Guide for Nursing Intervention and Patient Educationwawing16Noch keine Bewertungen
- Antidepressant DrugsDokument47 SeitenAntidepressant DrugsOjambo Flavia100% (3)
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDokument29 SeitenPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNoch keine Bewertungen
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDokument35 SeitenMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- Antidepressant Use in Adults With Chronic Kidney DiseaseDokument1 SeiteAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Psych Menmonics (Random)Dokument22 SeitenPsych Menmonics (Random)Kaly RieNoch keine Bewertungen
- How Inflammation May Cause Depression and Lead to New TreatmentsDokument12 SeitenHow Inflammation May Cause Depression and Lead to New Treatmentssimas100% (1)
- Provisional: Borderline Personality Disorder Differential DXDokument6 SeitenProvisional: Borderline Personality Disorder Differential DXhernandez2812Noch keine Bewertungen
- Psychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDokument80 SeitenPsychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDennis RagudoNoch keine Bewertungen
- Drugs Used in Mental IllnessDokument60 SeitenDrugs Used in Mental IllnessDixa MeNoch keine Bewertungen
- Overview of Psychotropic DrugsDokument7 SeitenOverview of Psychotropic Drugsnad101Noch keine Bewertungen
- (50 Studies Every Doctor Should Know) Ish P. Bhalla, Rajesh R. Tampi, Vinod H. Srihari - 50 Studies Every Psychiatrist Should Know-Oxford University Press (2018)Dokument374 Seiten(50 Studies Every Doctor Should Know) Ish P. Bhalla, Rajesh R. Tampi, Vinod H. Srihari - 50 Studies Every Psychiatrist Should Know-Oxford University Press (2018)Francisco VillalonNoch keine Bewertungen
- Lecture 4, Antipsychotics, AntidepressantsDokument94 SeitenLecture 4, Antipsychotics, Antidepressantsj.doe.hex_87100% (3)
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDokument8 SeitenCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNoch keine Bewertungen
- INTRODUCTION TO NEUROPHARMACOLOGYyyDokument27 SeitenINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviNoch keine Bewertungen
- PsychopharmacologyDokument50 SeitenPsychopharmacologyapi-3703352Noch keine Bewertungen
- SchizophreniaDokument22 SeitenSchizophrenianabeelNoch keine Bewertungen
- Current Clinical Strategies: Handbook of Psychiatric DrugsDokument72 SeitenCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Noch keine Bewertungen
- Psychotropic Drugs: Bryan Mae H. DegorioDokument65 SeitenPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Ferna-Case AnalysisDokument13 SeitenFerna-Case Analysisbea pegadNoch keine Bewertungen
- AntipsychoticsDokument29 SeitenAntipsychoticsTyler Lawrence Coye100% (4)
- Anidepressant Drugs: Pratik KhanalDokument37 SeitenAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- PsychopharmacologyDokument148 SeitenPsychopharmacologyAsther Mantua100% (2)
- The Food Mood Connection (Uma Naidoo MD)Dokument317 SeitenThe Food Mood Connection (Uma Naidoo MD)Adriana Ionita100% (1)
- Antidepressant Therapy AlgorithmDokument12 SeitenAntidepressant Therapy AlgorithmZubair Mahmood KamalNoch keine Bewertungen
- Soumya Mary 1 Year MSC (N)Dokument24 SeitenSoumya Mary 1 Year MSC (N)Salman HabeebNoch keine Bewertungen
- Antipsychotic DrugsDokument44 SeitenAntipsychotic DrugsPaulus Widjanarko Brotosaputro0% (1)
- B2B Psychopharmacology 2015Dokument128 SeitenB2B Psychopharmacology 2015Soleil DaddouNoch keine Bewertungen
- PHARMACOLOGY OF PSYCHOSIS AND MANIADokument53 SeitenPHARMACOLOGY OF PSYCHOSIS AND MANIAlavanyakakarlaNoch keine Bewertungen
- Antidepressant DrugsDokument41 SeitenAntidepressant DrugsSashaKay100% (5)
- Pharmacology in PsychiatryDokument33 SeitenPharmacology in PsychiatryKatrina PonceNoch keine Bewertungen
- Antidepressants and Mood StabilizersDokument4 SeitenAntidepressants and Mood Stabilizers우정은Noch keine Bewertungen
- PSYCHOPHARMACOLOGYDokument2 SeitenPSYCHOPHARMACOLOGYJulia Rae Delos SantosNoch keine Bewertungen
- AntidepressantsDokument4 SeitenAntidepressantsSalman HabeebNoch keine Bewertungen
- Psychiatric Nursing Documentation MethodsDokument25 SeitenPsychiatric Nursing Documentation MethodsMichelle ErikaNoch keine Bewertungen
- (Compact Research - Diseases and Disorders) Scott Barbour - Post-Traumatic Stress Disorder-ReferencePoint Press (2012)Dokument104 Seiten(Compact Research - Diseases and Disorders) Scott Barbour - Post-Traumatic Stress Disorder-ReferencePoint Press (2012)NOBELDINoch keine Bewertungen
- Inability To Bear Down: Problems With The Psyche FactorsDokument4 SeitenInability To Bear Down: Problems With The Psyche FactorsErvina Luisa Delias CampusNoch keine Bewertungen
- Antipsychotics Mechanisms Indications SideEffectsDokument4 SeitenAntipsychotics Mechanisms Indications SideEffectsRana MuhammadNoch keine Bewertungen
- ANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsDokument21 SeitenANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsKashis SharmaNoch keine Bewertungen
- Presented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Dokument17 SeitenPresented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Akanksha KapoorNoch keine Bewertungen
- Mental Health Nursing Exam QuestionsDokument17 SeitenMental Health Nursing Exam QuestionsSubiVictorNoch keine Bewertungen
- Assessor Guide For Hospital/ Shco: Nabh-AgDokument13 SeitenAssessor Guide For Hospital/ Shco: Nabh-AgSubiVictorNoch keine Bewertungen
- NABH Policy For AdverseDecisions Issue2 PDFDokument11 SeitenNABH Policy For AdverseDecisions Issue2 PDFSubiVictorNoch keine Bewertungen
- Nabh Policy and Procedure For Surprise Visit To An Accredited/ Certified HcoDokument5 SeitenNabh Policy and Procedure For Surprise Visit To An Accredited/ Certified HcoSubiVictorNoch keine Bewertungen
- Agreement Approved NewDokument12 SeitenAgreement Approved NewVishnu Teja ReddyNoch keine Bewertungen
- Policies & Procedures For Assessment, Surveillance and Re-Assessment of HcoDokument16 SeitenPolicies & Procedures For Assessment, Surveillance and Re-Assessment of HcoSubiVictorNoch keine Bewertungen
- FeeStructure Revision2016 PDFDokument1 SeiteFeeStructure Revision2016 PDFSubiVictorNoch keine Bewertungen
- PDFDokument2 SeitenPDFSubiVictorNoch keine Bewertungen
- Mood Stabilizers BookletDokument20 SeitenMood Stabilizers Bookletrabiaa_48Noch keine Bewertungen
- Uwishin - The DietDokument16 SeitenUwishin - The DietharlandizzleNoch keine Bewertungen
- MCQ CollectionDokument12 SeitenMCQ CollectionTeslim RajiNoch keine Bewertungen
- Art. 4 - 921Dokument6 SeitenArt. 4 - 921aviralNoch keine Bewertungen
- Psychopharmacological AgentsDokument44 SeitenPsychopharmacological Agentsbazet49Noch keine Bewertungen
- 2000605-2 FOC 18 4s Critique FinalDokument65 Seiten2000605-2 FOC 18 4s Critique FinalAna ZahariaNoch keine Bewertungen
- Conduct Disorder Diagnosis and Treatment in Primar PDFDokument11 SeitenConduct Disorder Diagnosis and Treatment in Primar PDFhopeIshanzaNoch keine Bewertungen
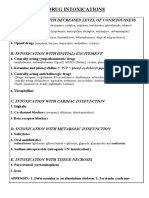
- Drug Intoxications: A. Intoxication With Decreased Level of ConsciousnessDokument22 SeitenDrug Intoxications: A. Intoxication With Decreased Level of ConsciousnessVika ShoniaNoch keine Bewertungen
- Treatment of Persistent Pain in Older Adults - Up to DateDokument25 SeitenTreatment of Persistent Pain in Older Adults - Up to DateMulya ImansyahNoch keine Bewertungen
- Falls in Older Persons - Risk Factors and Patient Evaluation - UpToDateDokument24 SeitenFalls in Older Persons - Risk Factors and Patient Evaluation - UpToDateNhungVũNoch keine Bewertungen
- Postpartum Psychiatric DisordersDokument55 SeitenPostpartum Psychiatric DisordersAklile TsegaNoch keine Bewertungen
- Ppi Guidance Apr 17 Post GWH CommentsDokument4 SeitenPpi Guidance Apr 17 Post GWH CommentsAnonymous MRcQuQODNoch keine Bewertungen
- Psychiatry MCQs 2Dokument11 SeitenPsychiatry MCQs 2Majed Alami100% (1)
- 1 Mood Disorders Whole Document 1Dokument10 Seiten1 Mood Disorders Whole Document 1Myles Zen Dieta EaNoch keine Bewertungen
- Obsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanDokument5 SeitenObsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanRidwan AdiansyahNoch keine Bewertungen
- Whitman Express 02 - 17 - 2011Dokument24 SeitenWhitman Express 02 - 17 - 2011Express EditorNoch keine Bewertungen
- Developmental Origins of Anxiety: A ReviewDokument8 SeitenDevelopmental Origins of Anxiety: A ReviewSnehaNoch keine Bewertungen
- Report On Obsessive-Compulsive-Disorders-and-Trauma-related-DisordersDokument42 SeitenReport On Obsessive-Compulsive-Disorders-and-Trauma-related-DisordersMatteo BayotNoch keine Bewertungen
- Jurnal Internasional MenopauseDokument8 SeitenJurnal Internasional MenopauseLembang DamariansyahNoch keine Bewertungen
- Polypharmacy in The ElderlyDokument9 SeitenPolypharmacy in The ElderlyTugasbu CicikNoch keine Bewertungen
- "Fake It Till You Make It"! Contaminating Rubber Hands ("Multisensory Stimulation Therapy") To Treat Obsessive-Compulsive DisorderDokument16 Seiten"Fake It Till You Make It"! Contaminating Rubber Hands ("Multisensory Stimulation Therapy") To Treat Obsessive-Compulsive DisorderSol PennisiNoch keine Bewertungen