Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Character FirstDokument10 SeitenCharacter FirstNatalia VeermanNoch keine Bewertungen
- 5 - Surah Al MaidahDokument98 Seiten5 - Surah Al MaidahmostromNoch keine Bewertungen
- Questions Which May Be Subject of Judicial ReviewDokument3 SeitenQuestions Which May Be Subject of Judicial ReviewCeline CabadingNoch keine Bewertungen
- Sienes vs. EsparciaDokument1 SeiteSienes vs. EsparciasamontedianneNoch keine Bewertungen
- Paradox and Challenges in Military Leadership An Israelian ApproachDokument30 SeitenParadox and Challenges in Military Leadership An Israelian Approachdorupara718747100% (1)
- Political Law A. The Constitution Definition, Nature and ConceptsDokument284 SeitenPolitical Law A. The Constitution Definition, Nature and ConceptsFairyssa Bianca SagotNoch keine Bewertungen
- Majorstatewise FY 2021Dokument121 SeitenMajorstatewise FY 2021Vishnu Varthanan LNoch keine Bewertungen
- January Task of The MonthDokument1 SeiteJanuary Task of The MonthinsccapNoch keine Bewertungen
- Weatherization TrainingDokument1 SeiteWeatherization TraininginsccapNoch keine Bewertungen
- February Task of The MonthDokument1 SeiteFebruary Task of The MonthinsccapNoch keine Bewertungen
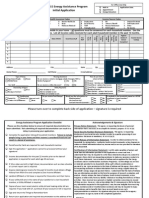
- 2015 Energy Assistance Program ApplicationDokument2 Seiten2015 Energy Assistance Program ApplicationinsccapNoch keine Bewertungen
- Holiday Assistance Application 2014Dokument1 SeiteHoliday Assistance Application 2014insccapNoch keine Bewertungen
- Landlord AffidavitDokument1 SeiteLandlord AffidavitinsccapNoch keine Bewertungen
- Foundations Award $406,000 in Grants To Local Projects: 1 CommentDokument9 SeitenFoundations Award $406,000 in Grants To Local Projects: 1 CommentinsccapNoch keine Bewertungen
- School Garage Sale FlyerDokument1 SeiteSchool Garage Sale FlyerinsccapNoch keine Bewertungen
- Growing Opportunities - SUPARpublicreportDokument13 SeitenGrowing Opportunities - SUPARpublicreportinsccapNoch keine Bewertungen
- Family Self-Sufficiency & Homeownership Programs: FSS & HOP Participant Brag WallDokument6 SeitenFamily Self-Sufficiency & Homeownership Programs: FSS & HOP Participant Brag WallinsccapNoch keine Bewertungen
- Ebus BloomingtonDokument1 SeiteEbus BloomingtoninsccapNoch keine Bewertungen
- Professional DisclosureDokument4 SeitenProfessional Disclosureapi-354945638Noch keine Bewertungen
- Dorian Yates 1987-1992 Workout Routine SpreadsheetDokument13 SeitenDorian Yates 1987-1992 Workout Routine SpreadsheetRicardo RibeiroNoch keine Bewertungen
- The CEO of Starbucks CaseDokument9 SeitenThe CEO of Starbucks CaseRyan DarcyNoch keine Bewertungen
- Character Traits and Black Beauty PageDokument1 SeiteCharacter Traits and Black Beauty PageROSE ZEYDELISNoch keine Bewertungen
- Full Manpower Satorp ProjectDokument4 SeitenFull Manpower Satorp ProjectBenjie dela RosaNoch keine Bewertungen
- Pro-Ante AgreementDokument1 SeitePro-Ante AgreementAmber NicosiaNoch keine Bewertungen
- Project Snowblind - Manual - PS2 PDFDokument15 SeitenProject Snowblind - Manual - PS2 PDFJasonNoch keine Bewertungen
- Case DigestDokument2 SeitenCase DigestBHEJAY ORTIZNoch keine Bewertungen
- TranscriptDokument3 SeitenTranscriptAaron J.Noch keine Bewertungen
- People V EscordialDokument24 SeitenPeople V Escordialanonymous0914Noch keine Bewertungen
- Diffie Hellman AlgorithmDokument11 SeitenDiffie Hellman Algorithmjoxy johnNoch keine Bewertungen
- Divorce Essay Final 15Dokument4 SeitenDivorce Essay Final 15api-307826848Noch keine Bewertungen
- 260 Supreme Court Reports Annotated: Cuartero vs. Court of AppealsDokument9 Seiten260 Supreme Court Reports Annotated: Cuartero vs. Court of AppealsFatima MagsinoNoch keine Bewertungen
- Transit Bail Referred To Full Bench 417240Dokument37 SeitenTransit Bail Referred To Full Bench 417240gaurang1984Noch keine Bewertungen
- Brimite v. United States of America - Document No. 14Dokument2 SeitenBrimite v. United States of America - Document No. 14Justia.comNoch keine Bewertungen
- LIMITATION ACT ProjectDokument22 SeitenLIMITATION ACT ProjectHARSH KUMARNoch keine Bewertungen
- The Sopranos - Complete 1st Season (DVDRip - Xvid) (h33t) (Big - Dad - E)Dokument3 SeitenThe Sopranos - Complete 1st Season (DVDRip - Xvid) (h33t) (Big - Dad - E)Canea VasileNoch keine Bewertungen
- NCLC Digital Library - 3.3.9.5 No Litigation Exemption - 2019-02-19Dokument1 SeiteNCLC Digital Library - 3.3.9.5 No Litigation Exemption - 2019-02-19Marie McDonnellNoch keine Bewertungen
- Claim Period or Limitation PeriodDokument3 SeitenClaim Period or Limitation PeriodIndranil RudraNoch keine Bewertungen
- Seno, Mendoza, Ruiz and Associates For Petitioner. Diores and Escareal Law Office For RespondentsDokument36 SeitenSeno, Mendoza, Ruiz and Associates For Petitioner. Diores and Escareal Law Office For RespondentsJayNoch keine Bewertungen
- UAPSA ChaptersDokument7 SeitenUAPSA ChaptersHarvin Julius LasqueroNoch keine Bewertungen
- 111 Alert Security and Investigation Agency Vs Saidali Pasawilan G.R. No. 182397Dokument6 Seiten111 Alert Security and Investigation Agency Vs Saidali Pasawilan G.R. No. 182397SDN HelplineNoch keine Bewertungen
- AKI MAN MovelistDokument3 SeitenAKI MAN MovelistShi YüanNoch keine Bewertungen