Das könnte Ihnen auch gefallen
- Norma Nfpa 2010Dokument40 SeitenNorma Nfpa 2010chebas2005Noch keine Bewertungen
- Circuit Protection in Healthcare FacilitiesDokument43 SeitenCircuit Protection in Healthcare FacilitiesMenaNoch keine Bewertungen
- CSA z32 Section 51Dokument8 SeitenCSA z32 Section 51Matt ThomasNoch keine Bewertungen
- Electricity System For HospitalsDokument14 SeitenElectricity System For HospitalsTejinderNoch keine Bewertungen
- API 570 - Closed Book Test - 334 TermsDokument17 SeitenAPI 570 - Closed Book Test - 334 TermsRizwan NazirNoch keine Bewertungen
- Medical Gas Piping SpecDokument22 SeitenMedical Gas Piping Specvvg100% (1)
- Patient Wall Systems ConfigurationDokument11 SeitenPatient Wall Systems Configurationno nameNoch keine Bewertungen
- Medical Gas Systems InstallationDokument8 SeitenMedical Gas Systems InstallationHermi DavidNoch keine Bewertungen
- Compliance: Waiting Areas Open To The CorridorDokument4 SeitenCompliance: Waiting Areas Open To The CorridorAFCONMEPNoch keine Bewertungen
- API 570, Piping Inspection Code (June 2006) .: (DAY 2 - Sections 1 To 6)Dokument5 SeitenAPI 570, Piping Inspection Code (June 2006) .: (DAY 2 - Sections 1 To 6)vishal bailur100% (1)
- Summlary of Safety and Effectiveness: 510 (K) SUMMVARYDokument10 SeitenSummlary of Safety and Effectiveness: 510 (K) SUMMVARYSurendar KesavanNoch keine Bewertungen
- Patient Grounding ModuleDokument4 SeitenPatient Grounding ModuleOliver HermosaNoch keine Bewertungen
- Ultra Clean Operating TheatreDokument6 SeitenUltra Clean Operating Theatreyogi_rulz_4evaNoch keine Bewertungen
- Is.13580.Internal Fuses &internal Overpressure Disconnectors For Power Electronic CapacitorsDokument12 SeitenIs.13580.Internal Fuses &internal Overpressure Disconnectors For Power Electronic CapacitorsSrikanth VoletiNoch keine Bewertungen
- National Electrical Code of The PhilippinesDokument5 SeitenNational Electrical Code of The PhilippinesRuzel AmpoanNoch keine Bewertungen
- Ref Book HV Bushings CH 2 StandardsDokument19 SeitenRef Book HV Bushings CH 2 StandardsShahid IqbalNoch keine Bewertungen
- Health Care Facilities PDFDokument12 SeitenHealth Care Facilities PDFshaaban2009Noch keine Bewertungen
- Laboratory Construction AppendicesDokument24 SeitenLaboratory Construction AppendicesLizbeth SalazarNoch keine Bewertungen
- ASA Publications Anesthesia Machine Obsolescence 20041Dokument7 SeitenASA Publications Anesthesia Machine Obsolescence 20041Julio Corona100% (1)
- Mechanical VentilationDokument48 SeitenMechanical VentilationAbeeesy AmrakeyNoch keine Bewertungen
- Eli Bulletin Ocpd CoordinationDokument1 SeiteEli Bulletin Ocpd CoordinationAirep OiralihNoch keine Bewertungen
- 2005 Nec ChangesDokument20 Seiten2005 Nec ChangesFlorabel Tolentino Sera JosefNoch keine Bewertungen
- Electrical Safety in Motor Maintenance and TestingDokument9 SeitenElectrical Safety in Motor Maintenance and Testingmte1Noch keine Bewertungen
- Electrical Safety in Motor MaintenanceDokument9 SeitenElectrical Safety in Motor Maintenanceadi nugrohoNoch keine Bewertungen
- Eia 364-21D 2008Dokument16 SeitenEia 364-21D 2008hadiranji40% (1)
- ENTC 4350: Electrical SafetyDokument91 SeitenENTC 4350: Electrical SafetyPriya WeraheraNoch keine Bewertungen
- 15 Saip 50Dokument5 Seiten15 Saip 50malika_00Noch keine Bewertungen
- Presentation MED 2011Dokument44 SeitenPresentation MED 2011altugNoch keine Bewertungen
- Switchgear Specification For High Voltage Switchgears CT PT BreakerDokument26 SeitenSwitchgear Specification For High Voltage Switchgears CT PT BreakerSumit TyagiNoch keine Bewertungen
- Consultant Specification Capitole 40Dokument12 SeitenConsultant Specification Capitole 40ericNoch keine Bewertungen
- Ansi MV Techtopics79 enDokument3 SeitenAnsi MV Techtopics79 enHaroon ZafarNoch keine Bewertungen
- ISO_10651-3_1997Dokument38 SeitenISO_10651-3_1997somenameNoch keine Bewertungen
- LPG and Electrical InstallationsDokument10 SeitenLPG and Electrical InstallationsNicolas150956Noch keine Bewertungen
- NFPA 99 ChangesDokument8 SeitenNFPA 99 ChangescarlcrowNoch keine Bewertungen
- Qcs 2010 Section 10 Part 3 Primary ElementsDokument9 SeitenQcs 2010 Section 10 Part 3 Primary Elementsbryanpastor106Noch keine Bewertungen
- Hager Isolators SwitchesDokument12 SeitenHager Isolators SwitchesDhanTimNoch keine Bewertungen
- 22 61 13 Compressed-Air Piping For Lab-HealthCare FacilitiesDokument16 Seiten22 61 13 Compressed-Air Piping For Lab-HealthCare FacilitiesKaruna KaranNoch keine Bewertungen
- 19 - Duct Mount Kit For H2S Detector - 975-000020-891 PDFDokument8 Seiten19 - Duct Mount Kit For H2S Detector - 975-000020-891 PDFjosephNoch keine Bewertungen
- Datasheet API Standard 53Dokument7 SeitenDatasheet API Standard 53LeonardoVianna100% (1)
- 33KV GTP WbsebDokument13 Seiten33KV GTP Wbsebmaniking1Noch keine Bewertungen
- Electrical RequirementsDokument55 SeitenElectrical RequirementsJerry MonteroNoch keine Bewertungen
- Electromagnetic Compatibility: EMC For Product Committees: A Short Guide To IEC Guide 107Dokument6 SeitenElectromagnetic Compatibility: EMC For Product Committees: A Short Guide To IEC Guide 107reza mirzakhaniNoch keine Bewertungen
- Design Criteria For Control System and InstrumentationDokument29 SeitenDesign Criteria For Control System and InstrumentationkamelkolsiNoch keine Bewertungen
- Modern Hospital Lifeline: Medical Gas Distribution SystemDokument4 SeitenModern Hospital Lifeline: Medical Gas Distribution SystemDurjoy_Sarker_143450% (2)
- Operating Instructions: OPTISWITCH 5100 C, 5150 C With Relay OutputDokument32 SeitenOperating Instructions: OPTISWITCH 5100 C, 5150 C With Relay OutputJose Mario Ferreyra MoranNoch keine Bewertungen
- Rapidly Manufactured Ventilator System Specification - GOV - UKDokument7 SeitenRapidly Manufactured Ventilator System Specification - GOV - UKMohammed AttiaNoch keine Bewertungen
- Heidelberg HRT3 - Installation ManualDokument29 SeitenHeidelberg HRT3 - Installation ManualZeljko TomicNoch keine Bewertungen
- Manejadora Lennox Cbx25 IomDokument16 SeitenManejadora Lennox Cbx25 IomNarcisoNoch keine Bewertungen
- PEC Assignment ExplainedDokument7 SeitenPEC Assignment ExplainedJon Lester CabanesNoch keine Bewertungen
- Ict 1000 Series: Hydrostatic Level Transmitter Installation Operation & Maintenance Instruction ManualDokument16 SeitenIct 1000 Series: Hydrostatic Level Transmitter Installation Operation & Maintenance Instruction ManualZer0GNoch keine Bewertungen
- J C. W, CHC, PMP, CMGV C M G S: Changes in The Medical Gas and Vacuum System RequirementsDokument119 SeitenJ C. W, CHC, PMP, CMGV C M G S: Changes in The Medical Gas and Vacuum System RequirementsCarmenDominguezJaraNoch keine Bewertungen
- ManualDokument56 SeitenManualam02Noch keine Bewertungen
- NR2 Lon Handbook PDFDokument68 SeitenNR2 Lon Handbook PDFsaturnerNoch keine Bewertungen
- Measuring cleanroom particle concentrationsDokument1 SeiteMeasuring cleanroom particle concentrationsramfajgeNoch keine Bewertungen
- US FDA Microwave Radiation HazardsDokument13 SeitenUS FDA Microwave Radiation HazardsPerry LanghamNoch keine Bewertungen
- ZEC310 Zone Damper and BYP200 Bypass Damper Controllers: Installation InstructionsDokument15 SeitenZEC310 Zone Damper and BYP200 Bypass Damper Controllers: Installation InstructionsRyn YahuFNoch keine Bewertungen
- 2 Cable Trunking and DuctsDokument8 Seiten2 Cable Trunking and Ductsaanouar77Noch keine Bewertungen
- 16th Edition IEE Wiring Regulations: Design and Verification of Electrical InstallationsVon Everand16th Edition IEE Wiring Regulations: Design and Verification of Electrical InstallationsBewertung: 4 von 5 Sternen4/5 (1)
- The IEE Wiring Regulations Explained and IllustratedVon EverandThe IEE Wiring Regulations Explained and IllustratedBewertung: 4 von 5 Sternen4/5 (14)
- THEORIES OF CONSUMER BEHAVIOUR EXPLAINEDDokument45 SeitenTHEORIES OF CONSUMER BEHAVIOUR EXPLAINEDShishan AhmadNoch keine Bewertungen
- Consumer Attitude Metrics For Guiding Marketing Mix DecisionsDokument18 SeitenConsumer Attitude Metrics For Guiding Marketing Mix DecisionsShishan AhmadNoch keine Bewertungen
- By Harshitha.S and Imran PashaDokument41 SeitenBy Harshitha.S and Imran PashaShishan AhmadNoch keine Bewertungen
- Coca Cola Decision MakingDokument7 SeitenCoca Cola Decision MakingShishan AhmadNoch keine Bewertungen
- Social Science & Medicine: Sarah Durkin, Megan Bayly, Trish Cotter, Sandra Mullin, Melanie Wake FieldDokument10 SeitenSocial Science & Medicine: Sarah Durkin, Megan Bayly, Trish Cotter, Sandra Mullin, Melanie Wake FieldShishan AhmadNoch keine Bewertungen
- Prospect Theory and Liquidation DecisionsDokument16 SeitenProspect Theory and Liquidation DecisionsShishan AhmadNoch keine Bewertungen
- Behavioral Finance in Brazil: Applying The Prospect Theory To Potential InvestorsDokument22 SeitenBehavioral Finance in Brazil: Applying The Prospect Theory To Potential InvestorsShishan AhmadNoch keine Bewertungen
- Impact of Anti Smoking Campaigns On Youth Impact of Anti Smoking Campaigns On YouthDokument8 SeitenImpact of Anti Smoking Campaigns On Youth Impact of Anti Smoking Campaigns On YouthShishan AhmadNoch keine Bewertungen
- Do Financial Professionals Behave According To Prospect Theory? An Experimental StudyDokument19 SeitenDo Financial Professionals Behave According To Prospect Theory? An Experimental StudyShishan AhmadNoch keine Bewertungen
- Journal of Services Marketing: Article InformationDokument17 SeitenJournal of Services Marketing: Article InformationShishan AhmadNoch keine Bewertungen
- 02 Chapter 2Dokument60 Seiten02 Chapter 2swapnshriNoch keine Bewertungen
- Impact of Anti Smoking Campaigns On Youth Impact of Anti Smoking Campaigns On YouthDokument8 SeitenImpact of Anti Smoking Campaigns On Youth Impact of Anti Smoking Campaigns On YouthShishan AhmadNoch keine Bewertungen
- Thun Holm 2004Dokument14 SeitenThun Holm 2004Shishan AhmadNoch keine Bewertungen
- The Efficacy of Anti-Smoking Advertisements: The Role of Source, Message, and Individual CharacteristicsDokument14 SeitenThe Efficacy of Anti-Smoking Advertisements: The Role of Source, Message, and Individual CharacteristicsShishan AhmadNoch keine Bewertungen
- The Graphic Side of Fear - The Effects of Anti-Tobacco Graphic THRDokument129 SeitenThe Graphic Side of Fear - The Effects of Anti-Tobacco Graphic THRShishan AhmadNoch keine Bewertungen
- Pre-Feasibility Study on UPVC Pipe Manufacturing UnitDokument21 SeitenPre-Feasibility Study on UPVC Pipe Manufacturing UnitShishan AhmadNoch keine Bewertungen
- Effectiveness of Anti Smoking AdvertisinDokument8 SeitenEffectiveness of Anti Smoking AdvertisinShishan AhmadNoch keine Bewertungen
- Fear Appeals Anti Smoking JMM Feb11 Final ResubmissionDokument37 SeitenFear Appeals Anti Smoking JMM Feb11 Final ResubmissionShishan AhmadNoch keine Bewertungen
- KAS General CatalogDokument64 SeitenKAS General CatalogShishan AhmadNoch keine Bewertungen
- Consumer Behavior Main Assignment 1Dokument22 SeitenConsumer Behavior Main Assignment 1Shishan AhmadNoch keine Bewertungen
- Coca Cola Decision MakingDokument7 SeitenCoca Cola Decision MakingShishan AhmadNoch keine Bewertungen
- Bachelor Thesis 2012Dokument58 SeitenBachelor Thesis 2012Shishan AhmadNoch keine Bewertungen
- 01148Dokument4 Seiten01148paresh131Noch keine Bewertungen
- G BrassFittingsDokument22 SeitenG BrassFittingsC_a_RNoch keine Bewertungen
- 01148Dokument4 Seiten01148paresh131Noch keine Bewertungen
- 79 - CP Angle ValveDokument1 Seite79 - CP Angle ValveShishan AhmadNoch keine Bewertungen
- Caleffi: Thermostatic Mixing Valve With Interchangeable Cartridge For Centralised SystemsDokument4 SeitenCaleffi: Thermostatic Mixing Valve With Interchangeable Cartridge For Centralised SystemsShishan AhmadNoch keine Bewertungen
- 78 Soft Seat Chromium Plated Brass Angle Valve: by PeglerDokument1 Seite78 Soft Seat Chromium Plated Brass Angle Valve: by PeglerShishan AhmadNoch keine Bewertungen
- Thermostatic mixing valve installation guideDokument18 SeitenThermostatic mixing valve installation guideShishan AhmadNoch keine Bewertungen
- Bronze Safety Relief Valve: SV-B27 SVP-B27 SV-B29 SVP-B29Dokument1 SeiteBronze Safety Relief Valve: SV-B27 SVP-B27 SV-B29 SVP-B29Shishan Ahmad100% (1)
- Service Bulletins,: For Manipulator Systems, Slave Arms, & AccessoriesDokument44 SeitenService Bulletins,: For Manipulator Systems, Slave Arms, & AccessoriesKenneth S.Noch keine Bewertungen
- SECURITY GLAZINGDokument11 SeitenSECURITY GLAZINGjack.simpson.changNoch keine Bewertungen
- 10 Steps To A Better Rheological Measurement PDFDokument44 Seiten10 Steps To A Better Rheological Measurement PDFHílary VpbNoch keine Bewertungen
- Construction Solutions - Jindal Steel & Power LTDDokument29 SeitenConstruction Solutions - Jindal Steel & Power LTDjindalsteelsNoch keine Bewertungen
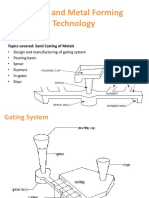
- Sand Casting Guide: Gating Systems & RisersDokument31 SeitenSand Casting Guide: Gating Systems & RisersAmruta Rane100% (1)
- Designguide Ankre 0408Dokument152 SeitenDesignguide Ankre 0408Federico.IoriNoch keine Bewertungen
- Catalog Web SlingsDokument39 SeitenCatalog Web SlingsMichel NdiayeNoch keine Bewertungen
- Design of Composite ColumnsDokument7 SeitenDesign of Composite Columnsabozaid19Noch keine Bewertungen
- 3.3 - Lockhart & Crescenzi - Sour Oil and Gas Management PDFDokument34 Seiten3.3 - Lockhart & Crescenzi - Sour Oil and Gas Management PDFsantiagoNoch keine Bewertungen
- Calcium Silicate Bricks or Sand Lime BricksDokument4 SeitenCalcium Silicate Bricks or Sand Lime Bricksmanhal alnoaimyNoch keine Bewertungen
- En Tool Clamping Systems 2012Dokument72 SeitenEn Tool Clamping Systems 2012Goran MiodragovicNoch keine Bewertungen
- Degradation and Preservation Methods of Timber StructuresDokument24 SeitenDegradation and Preservation Methods of Timber StructuresLórántBirtalanNoch keine Bewertungen
- Four Mark Question Answers Chapter Wise Value Based QuestionsDokument3 SeitenFour Mark Question Answers Chapter Wise Value Based QuestionsnitishNoch keine Bewertungen
- Gearbox 001 PDFDokument178 SeitenGearbox 001 PDFmagelan100% (1)
- Chapter 2 Multiple-Choice QuestionsDokument8 SeitenChapter 2 Multiple-Choice QuestionsDavid LouNoch keine Bewertungen
- C87600 Copper Silicon: Brass & Bronze AlloysDokument1 SeiteC87600 Copper Silicon: Brass & Bronze AlloysDeepak KumarNoch keine Bewertungen
- Aalco Metals LTD Aluminium AlloyDokument2 SeitenAalco Metals LTD Aluminium Alloyanwarali1975Noch keine Bewertungen
- Mark Schemes Summer 2008: IGCSE Chemistry (4335)Dokument27 SeitenMark Schemes Summer 2008: IGCSE Chemistry (4335)EZNoch keine Bewertungen
- TV SERVICE MANUAL GUIDEDokument49 SeitenTV SERVICE MANUAL GUIDEXNicolasx XGomezxNoch keine Bewertungen
- CNC Training Program IntroductionDokument248 SeitenCNC Training Program IntroductionJuan100% (1)
- 2009-12-29 224215 01 Escape Steering Squeek TSB 06-23-03Dokument2 Seiten2009-12-29 224215 01 Escape Steering Squeek TSB 06-23-03Randy SmithNoch keine Bewertungen
- 3.0. CementDokument10 Seiten3.0. CementJohn luckyNoch keine Bewertungen
- XT702PDokument3 SeitenXT702PBDMNoch keine Bewertungen
- Material & Consumables RequirementsDokument6 SeitenMaterial & Consumables RequirementsDoc TorNoch keine Bewertungen
- SSP Nfra BDT1 Jind MST 00032Dokument42 SeitenSSP Nfra BDT1 Jind MST 00032Zulhazmi ZulkafliNoch keine Bewertungen
- Csa Rotordryer PDFDokument8 SeitenCsa Rotordryer PDFpeterpunk75Noch keine Bewertungen
- TB1-019 Off-Line Boiler Protection OptionsDokument1 SeiteTB1-019 Off-Line Boiler Protection Optionsjesus_manrique2753Noch keine Bewertungen
- LM2500 Course PDFDokument86 SeitenLM2500 Course PDFKorichiKarim100% (9)
- Rochor Station Pile Design CalculationsDokument15 SeitenRochor Station Pile Design CalculationsDifa LiuNoch keine Bewertungen