Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Basic of Geriatrics and Internal Medicine For PhysiotherapistDokument128 SeitenBasic of Geriatrics and Internal Medicine For PhysiotherapistDoha EbedNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Is She Depressed???.": What Is Your Differential Diagnosis What Other Information Would You Like To Know About Mrs. X ?Dokument5 SeitenIs She Depressed???.": What Is Your Differential Diagnosis What Other Information Would You Like To Know About Mrs. X ?Doha EbedNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Percutaneous Endoscopic GastrostomyDokument27 SeitenPercutaneous Endoscopic GastrostomyDoha EbedNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Univ LawDokument201 SeitenUniv LawTamer Farouk KhalifaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Drug DosingDokument83 SeitenDrug DosingDoha EbedNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- HeelDokument4 SeitenHeelDoha EbedNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Acid Base BalanceDokument20 SeitenAcid Base BalanceDoha Ebed100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- ProstatitisDokument23 SeitenProstatitisDoha Ebed100% (1)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Sleep Disturbances SleepDisturbancesinElderlyDokument104 SeitenSleep Disturbances SleepDisturbancesinElderlyDoha EbedNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Foot ProblemsDokument106 SeitenFoot ProblemsDoha EbedNoch keine Bewertungen
- Low Back Pain: Dr. Doha RasheedyDokument40 SeitenLow Back Pain: Dr. Doha RasheedyDoha EbedNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Multimorbidities in Older Adults With AFDokument5 SeitenMultimorbidities in Older Adults With AFDoha EbedNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Thickened Common Femoral Artery Intima Media Thickness: A Surrogate Marker For Subclinical Peripheral Arterial Disease in Patients With Type 2 Diabetes MellitusDokument4 SeitenThickened Common Femoral Artery Intima Media Thickness: A Surrogate Marker For Subclinical Peripheral Arterial Disease in Patients With Type 2 Diabetes MellitusDoha EbedNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Confidence IntervalsDokument1 SeiteConfidence IntervalsDoha EbedNoch keine Bewertungen
- OsteoporosisDokument7 SeitenOsteoporosisDoha EbedNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- 2013 Undergrad Med CurriculumDokument4 Seiten2013 Undergrad Med CurriculumDoha EbedNoch keine Bewertungen
- OsteoporosisDokument17 SeitenOsteoporosisDoha EbedNoch keine Bewertungen
- Social Cognition Profile in Amnestic MCIDokument5 SeitenSocial Cognition Profile in Amnestic MCIDoha EbedNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Social Cognition Profile in Amnestic MCIDokument5 SeitenSocial Cognition Profile in Amnestic MCIDoha EbedNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Kidney Disease in ElderlyDokument5 SeitenKidney Disease in ElderlyDoha EbedNoch keine Bewertungen
- Pneumonia SeverityDokument7 SeitenPneumonia SeverityDoha EbedNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Health Promotion ProgramDokument9 SeitenHealth Promotion ProgramDoha EbedNoch keine Bewertungen
- HRQOLDokument4 SeitenHRQOLDoha EbedNoch keine Bewertungen
- CGADokument29 SeitenCGADoha EbedNoch keine Bewertungen
- Management of Acute Renal FailureDokument8 SeitenManagement of Acute Renal FailureIVAN100% (1)
- Case Presentation DELIRIUMDokument14 SeitenCase Presentation DELIRIUMDoha EbedNoch keine Bewertungen
- BJA CEPD Reviews 2003 Halsall 5 9Dokument5 SeitenBJA CEPD Reviews 2003 Halsall 5 9Doha EbedNoch keine Bewertungen
- Fluids and ElectrolytesDokument48 SeitenFluids and ElectrolytesDoha EbedNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Clinical StatisticsDokument257 SeitenClinical Statisticsfatcode27Noch keine Bewertungen
- Evaluation and Management of Shock States: Hypovolemic, Distributive, and Cardiogenic ShockDokument17 SeitenEvaluation and Management of Shock States: Hypovolemic, Distributive, and Cardiogenic ShockMarest AskynaNoch keine Bewertungen
- Critical Illness: Nutrition Care ManualDokument20 SeitenCritical Illness: Nutrition Care ManualDiogo JuniorNoch keine Bewertungen
- 7 Dengue FeverDokument6 Seiten7 Dengue FeverNicole HipolNoch keine Bewertungen
- I Hi Severe Sepsis BundlesDokument59 SeitenI Hi Severe Sepsis BundlesPedro AliagaNoch keine Bewertungen
- Surgical Unit 3 BMCH: Badal KhanDokument74 SeitenSurgical Unit 3 BMCH: Badal KhanUzma KhanNoch keine Bewertungen
- American Family Physician - February 1, 2019 - Gastroenteritis in ChildrenDokument17 SeitenAmerican Family Physician - February 1, 2019 - Gastroenteritis in ChildrenDaniel PuertasNoch keine Bewertungen
- Acute Diarrhoea and VomitingDokument43 SeitenAcute Diarrhoea and VomitingAdriana AfiqahNoch keine Bewertungen
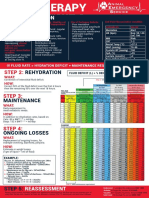
- AES - FluidChart 2020Dokument1 SeiteAES - FluidChart 2020Christian De Leon100% (1)
- 103 Dosage Chart - tcm1310-72815 PDFDokument1 Seite103 Dosage Chart - tcm1310-72815 PDFJaveria ShafiNoch keine Bewertungen
- Revision Cetoacidosis DiabeticaDokument15 SeitenRevision Cetoacidosis DiabeticaChristianNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Monografi CisplatinDokument11 SeitenMonografi CisplatinEmmaNoch keine Bewertungen
- Technologies For The Production of Pharmaceutical Grade Sodium ChlorideDokument13 SeitenTechnologies For The Production of Pharmaceutical Grade Sodium ChlorideAmyNoch keine Bewertungen
- A Guide To Improving The Care of Patients With Fragility Fractures, Edition 2Dokument63 SeitenA Guide To Improving The Care of Patients With Fragility Fractures, Edition 2Alejandro OrduzNoch keine Bewertungen
- Acute Viral Gastroenteritis in AdultsDokument13 SeitenAcute Viral Gastroenteritis in AdultsyessyNoch keine Bewertungen
- Fluid Management For The Pediatric Surgical Patient POWERPOINTDokument34 SeitenFluid Management For The Pediatric Surgical Patient POWERPOINTDipta Anggara100% (2)
- HII Coding Process GuideDokument3 SeitenHII Coding Process GuidePrashanthPatroNoch keine Bewertungen
- Burn ManagementDokument13 SeitenBurn Managementhendra ciptaNoch keine Bewertungen
- Bronquiolitis Grave Guías Francesas Enero 2023Dokument21 SeitenBronquiolitis Grave Guías Francesas Enero 2023TERAPEUTAS RESPIRATORIOS CLINVERNoch keine Bewertungen
- 04 FCH Acute GastroenteritisDokument9 Seiten04 FCH Acute GastroenteritisClar MoniquezNoch keine Bewertungen
- Diarrheal DiseasesDokument15 SeitenDiarrheal DiseasesAMOS MELINoch keine Bewertungen
- Dr. Nur Samsu, SPPD-KGH, FINASIM - ICD Pengenalan Dini Sepsis Di Layanan PrimerDokument37 SeitenDr. Nur Samsu, SPPD-KGH, FINASIM - ICD Pengenalan Dini Sepsis Di Layanan PrimerWahyu PurnamaNoch keine Bewertungen
- The Pathophysiology of Sepsis - 2021 Update - Part 2, Organ Dysfunction and AssessmentDokument13 SeitenThe Pathophysiology of Sepsis - 2021 Update - Part 2, Organ Dysfunction and AssessmentValerie ZimmermannNoch keine Bewertungen
- Gastro Inter It IsDokument3 SeitenGastro Inter It IsDhea Imas WijayantiNoch keine Bewertungen
- Fluid and Electrolyte in InfantDokument44 SeitenFluid and Electrolyte in InfantVibin K vNoch keine Bewertungen
- Fluids and ElectrolytesDokument48 SeitenFluids and ElectrolytesChernobyle Tolentino BattadNoch keine Bewertungen
- Obrien2013 PDFDokument11 SeitenObrien2013 PDFIrham AbsharNoch keine Bewertungen
- Salmonellosis: Odsigue, Clarissa Rama, Alea Albert Rosales, Joy SybilDokument36 SeitenSalmonellosis: Odsigue, Clarissa Rama, Alea Albert Rosales, Joy SybilAleya Albert RamaNoch keine Bewertungen
- Drug CalculationsDokument6 SeitenDrug CalculationsJB ReyesNoch keine Bewertungen
- Shock and Multisystem Failure: Rudolf M. TanDokument22 SeitenShock and Multisystem Failure: Rudolf M. TanDan Dan ManaoisNoch keine Bewertungen
- Burn Fluid ResuscitationDokument35 SeitenBurn Fluid ResuscitationNur Anniesa100% (2)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)