Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- T - Proc - Notices - Notices - 045 - K - Notice - Doc - 41757 - 870072414 EditDokument29 SeitenT - Proc - Notices - Notices - 045 - K - Notice - Doc - 41757 - 870072414 EdityusrieNoch keine Bewertungen
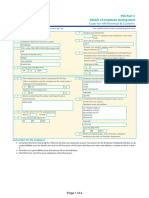
- O.P.C.F 16 Suspension of CoverageDokument1 SeiteO.P.C.F 16 Suspension of CoverageGarry sharmaNoch keine Bewertungen
- Handbook 2020-2021Dokument44 SeitenHandbook 2020-2021Dragomir PopaNoch keine Bewertungen
- Types of Insurance and Premium Comparison in PakistanDokument10 SeitenTypes of Insurance and Premium Comparison in PakistanSyed Baqar AliNoch keine Bewertungen
- Chapter V - Marine Insurance Practices of Marine InsuranceDokument3 SeitenChapter V - Marine Insurance Practices of Marine InsuranceMithunNoch keine Bewertungen
- Ryanair Travel ItineraryDokument5 SeitenRyanair Travel ItineraryJoanne CouplandNoch keine Bewertungen
- Health & Travel - February PointsDokument1 SeiteHealth & Travel - February Pointsnikksingh511Noch keine Bewertungen
- HealthInsurance-forIndiasMissingMiddle 28-10-2021 230116 211000Dokument65 SeitenHealthInsurance-forIndiasMissingMiddle 28-10-2021 230116 211000Amit PaliwalNoch keine Bewertungen
- 9704316Dokument105 Seiten9704316abhinav pachauriNoch keine Bewertungen
- Med, Supp, Adv Script Live TransferDokument3 SeitenMed, Supp, Adv Script Live TransferANA MARIE CANTARNoch keine Bewertungen
- Sanction Letter: Shop No 7 11 C Prince Plaza Sneha Nagar, Indore Indore, Madhya Pradesh, 452001Dokument7 SeitenSanction Letter: Shop No 7 11 C Prince Plaza Sneha Nagar, Indore Indore, Madhya Pradesh, 452001NISHA BANSALNoch keine Bewertungen
- Business Studies: Revision Booklet 2020 TERM 2 Grade 12Dokument25 SeitenBusiness Studies: Revision Booklet 2020 TERM 2 Grade 12Rabby KapelaNoch keine Bewertungen
- General Principles of Tort Law: Prof. Daniel Stein Aug, 2021Dokument14 SeitenGeneral Principles of Tort Law: Prof. Daniel Stein Aug, 2021Sidharth NambiarNoch keine Bewertungen
- Oona Corporate Profile - v16Dokument16 SeitenOona Corporate Profile - v16PFMPC SecretaryNoch keine Bewertungen
- Draft MOU Garage TieupDokument3 SeitenDraft MOU Garage Tieupjassi7nishad100% (1)
- Module 5 ProblemSheetDokument1 SeiteModule 5 ProblemSheetNikita ShakyaNoch keine Bewertungen
- Workb K: Financial EducationDokument51 SeitenWorkb K: Financial EducationRithishvel S SNoch keine Bewertungen
- VL Insurance Policy Withdrawal Surrender Request Form FillableDokument1 SeiteVL Insurance Policy Withdrawal Surrender Request Form FillableNew BossNoch keine Bewertungen
- Final2 - RBU - Guidelines For StudentsDokument23 SeitenFinal2 - RBU - Guidelines For StudentsYeeyan TanNoch keine Bewertungen
- B5952260 - Rahma Ali - Roble - P45 - 2324Dokument4 SeitenB5952260 - Rahma Ali - Roble - P45 - 2324rahmaroble71Noch keine Bewertungen
- Institute of Management Studies Davv Indore Mba (Financial Administration) Ii ND Semester - Fa 303C Insurance and Bank ManagementDokument2 SeitenInstitute of Management Studies Davv Indore Mba (Financial Administration) Ii ND Semester - Fa 303C Insurance and Bank ManagementjaiNoch keine Bewertungen
- Intro To Ratemaking SampleDokument51 SeitenIntro To Ratemaking SampleEvelyn JacquelineNoch keine Bewertungen
- Contract 2-Study HintsDokument9 SeitenContract 2-Study HintsRAJANoch keine Bewertungen
- Education Importance EssayDokument5 SeitenEducation Importance Essayxsfazwwhd100% (1)
- AINS 22 - Segment B Quiz (Qizlet)Dokument18 SeitenAINS 22 - Segment B Quiz (Qizlet)Karly Alleyne100% (1)
- Perfection Case DigestDokument5 SeitenPerfection Case DigestCy DacerNoch keine Bewertungen
- Ananya Rai Sbi LifeDokument129 SeitenAnanya Rai Sbi LifeNITISH CHANDRA PANDEYNoch keine Bewertungen
- BillPayments RaipurDokument19 SeitenBillPayments RaipurMukesh SinghNoch keine Bewertungen
- Kiara Jamison Insurance CardDokument1 SeiteKiara Jamison Insurance CardLillian AwtNoch keine Bewertungen
- Insurance Clauses in Construction Contracts: Insights April 2019Dokument14 SeitenInsurance Clauses in Construction Contracts: Insights April 2019yaserplNoch keine Bewertungen