Das könnte Ihnen auch gefallen
- 1Dokument4 Seiten1Dashari Ermandi HNoch keine Bewertungen
- Jadwal BHD RSKM SeptemberDokument3 SeitenJadwal BHD RSKM SeptemberDashari Ermandi HNoch keine Bewertungen
- Foto FotoDokument7 SeitenFoto FotoDashari Ermandi HNoch keine Bewertungen
- LK September 2019Dokument1 SeiteLK September 2019Dashari Ermandi HNoch keine Bewertungen
- Berita Acara April 2019Dokument1 SeiteBerita Acara April 2019Dashari Ermandi HNoch keine Bewertungen
- Absen Operasional SeptemberDokument10 SeitenAbsen Operasional SeptemberDashari Ermandi HNoch keine Bewertungen
- Absen Operasional 2019Dokument6 SeitenAbsen Operasional 2019Dashari Ermandi HNoch keine Bewertungen
- Harga Obat 250 OrgDokument5 SeitenHarga Obat 250 OrgDashari Ermandi HNoch keine Bewertungen
- Acute Coronary SyndromeDokument45 SeitenAcute Coronary SyndromeDashari Ermandi HNoch keine Bewertungen
- Harga Obat 250 OrgDokument5 SeitenHarga Obat 250 OrgDashari Ermandi HNoch keine Bewertungen
- Harga Obat 250 OrgDokument5 SeitenHarga Obat 250 OrgDashari Ermandi HNoch keine Bewertungen
- Follow Up: Tanggal 18-21 Mei 2014 S: Demam (-), Nyeri Pinggang (-) O: TD: 110/70 MMHGDokument2 SeitenFollow Up: Tanggal 18-21 Mei 2014 S: Demam (-), Nyeri Pinggang (-) O: TD: 110/70 MMHGDashari Ermandi HNoch keine Bewertungen
- Benign Conditions of The Thyroid Gland Just SeeDokument5 SeitenBenign Conditions of The Thyroid Gland Just SeeDashari Ermandi HNoch keine Bewertungen
- Nicemedia LiveDokument57 SeitenNicemedia LiveLawrence McleodNoch keine Bewertungen
- Hipertensi 1Dokument7 SeitenHipertensi 1Dashari Ermandi HNoch keine Bewertungen
- K13 Extrapyramydal DisorderDokument55 SeitenK13 Extrapyramydal DisorderDashari Ermandi HNoch keine Bewertungen
- Format Penilaian PelatihanDokument2 SeitenFormat Penilaian PelatihanDashari Ermandi HNoch keine Bewertungen
- Lampiran IraDokument3 SeitenLampiran IraDashari Ermandi HNoch keine Bewertungen
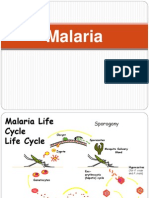
- K24 Baru Kuliah Malaria Blok TropmedDokument17 SeitenK24 Baru Kuliah Malaria Blok TropmedDashari Ermandi HNoch keine Bewertungen
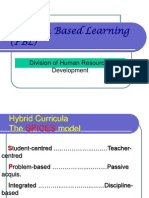
- K 2 - PBLDokument18 SeitenK 2 - PBLDashari Ermandi HNoch keine Bewertungen
- Cannulation 1Dokument5 SeitenCannulation 1TONY GO AWAYNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- FDS Amp 2020Dokument140 SeitenFDS Amp 2020Shahrukh ali khan100% (1)
- Bpacnz Antibiotics GuideDokument40 SeitenBpacnz Antibiotics GuideBulborea MihaelaNoch keine Bewertungen
- Pilonidal SinusDokument3 SeitenPilonidal SinusHaddani FozaNoch keine Bewertungen
- CM 86 192Dokument4 SeitenCM 86 192lucia pereiraNoch keine Bewertungen
- Prostatic Abscess - StatPearls - NCBI BookshelfDokument14 SeitenProstatic Abscess - StatPearls - NCBI BookshelfSheshang KamathNoch keine Bewertungen
- Intra-Abdominal Infections: Resident's Lecture Edward L. Goodman, MD May 1, 2006Dokument36 SeitenIntra-Abdominal Infections: Resident's Lecture Edward L. Goodman, MD May 1, 2006srweaverNoch keine Bewertungen
- TonsilitisDokument32 SeitenTonsilitisFitriNajibahNoch keine Bewertungen
- Infeksi Bahan KuliahDokument209 SeitenInfeksi Bahan KuliahIvi ChristinNoch keine Bewertungen
- Peritonsillar Abscess (Quinsy)Dokument18 SeitenPeritonsillar Abscess (Quinsy)Michael AmandyNoch keine Bewertungen
- The Zodiac and The Salts of SalvationDokument32 SeitenThe Zodiac and The Salts of Salvationrogerfpa100% (1)
- Mastitis 2Dokument25 SeitenMastitis 2Riana Pasca RoshianNoch keine Bewertungen
- Summary For Acute AppendicitisDokument13 SeitenSummary For Acute AppendicitisFemale calmNoch keine Bewertungen
- Orthopedic Infections, Osteomyelitis:Septic ArthritisDokument65 SeitenOrthopedic Infections, Osteomyelitis:Septic ArthritisnhfbyqvgwhNoch keine Bewertungen
- Surgical Protocols For Handling Covid-19 Positive PatientDokument4 SeitenSurgical Protocols For Handling Covid-19 Positive PatientInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Sae 2Dokument6 SeitenSae 2hardi adiyatmaNoch keine Bewertungen
- AbscessDokument5 SeitenAbscessJarotbemnkompinNoch keine Bewertungen
- What Is A Pilonidal Sinus, What Causes Them and What Are The Symptoms of Pilonidal SinusDokument4 SeitenWhat Is A Pilonidal Sinus, What Causes Them and What Are The Symptoms of Pilonidal SinusThavam RatnaNoch keine Bewertungen
- Brain AbscessDokument25 SeitenBrain AbscessprembarnabasNoch keine Bewertungen
- PDF Abses BezoldDokument5 SeitenPDF Abses BezoldNiia D'girlsNoch keine Bewertungen
- StaphDokument1 SeiteStaphPrabhjot Singh BakshiNoch keine Bewertungen
- Case Study FistulectomyDokument94 SeitenCase Study FistulectomynycharlzNoch keine Bewertungen
- Cellulitis Definition, Etiology, and Clinical FeaturesDokument10 SeitenCellulitis Definition, Etiology, and Clinical Featuresrosscharles1006869Noch keine Bewertungen
- Chapter-18 - Orofacial Infection and Its SpreadDokument6 SeitenChapter-18 - Orofacial Infection and Its Spreadbjahboi2Noch keine Bewertungen
- Homeopathic RemediesDokument15 SeitenHomeopathic Remediessaeedchaand100% (1)
- Brain AbscessDokument5 SeitenBrain AbscessEugene Briagas Roque100% (1)
- #Complications of Suppurative Otitis MediaDokument8 Seiten#Complications of Suppurative Otitis MediaameerabestNoch keine Bewertungen
- Management of ENT Emergencies: Simon Lloyd Consultant ENT Surgeon Central Manchester NHS Foundation TrustDokument52 SeitenManagement of ENT Emergencies: Simon Lloyd Consultant ENT Surgeon Central Manchester NHS Foundation TrustDzulkifli I. DotutinggiNoch keine Bewertungen
- Dermatology Chap6. Bacterial Infections of Skin 2020-3-23Dokument368 SeitenDermatology Chap6. Bacterial Infections of Skin 2020-3-23Mohsin Tanmoy100% (1)
- AppendicitisDokument16 SeitenAppendicitisFiras AbusharikhNoch keine Bewertungen
- Skin Pathology NotesDokument2 SeitenSkin Pathology NotesVanessa HermioneNoch keine Bewertungen