Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Part and Mold Design Guide (2005)Dokument174 SeitenPart and Mold Design Guide (2005)naitikpanchal100% (4)
- Cerebellum & Brain-Stem AnatomyDokument23 SeitenCerebellum & Brain-Stem AnatomyMuhammad ShahzaibNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Classic Beer Style Series #02 - Continental PilsnerDokument106 SeitenClassic Beer Style Series #02 - Continental PilsnerFred smith100% (1)
- Science Quiz Bee Grade 3Dokument4 SeitenScience Quiz Bee Grade 3Rhea B Borromeo100% (1)
- Monitoring Ecological ChangeDokument411 SeitenMonitoring Ecological ChangeSylvain O' Marinier75% (4)
- The Spark in The MachineDokument6 SeitenThe Spark in The MachineElanghovan ArumugamNoch keine Bewertungen
- Firefighter FitnessDokument13 SeitenFirefighter FitnessSeptimiu BotaNoch keine Bewertungen
- Development Stages of The Learner - FinalDokument80 SeitenDevelopment Stages of The Learner - FinalJeniffer Quiambao Tango-an100% (2)
- Crash Analysis 240509Dokument39 SeitenCrash Analysis 240509Jason RogersNoch keine Bewertungen
- Itp Piping PDFDokument4 SeitenItp Piping PDFdashNoch keine Bewertungen
- Booking Confirmation For Process Number 123782146Dokument2 SeitenBooking Confirmation For Process Number 123782146Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument3 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- Unbeatable forex rates contact FCM travel deskDokument2 SeitenUnbeatable forex rates contact FCM travel deskJason RogersNoch keine Bewertungen
- Letter 1Dokument1 SeiteLetter 1Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument2 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument3 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument2 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- Receipt 9862882Dokument1 SeiteReceipt 9862882Jason RogersNoch keine Bewertungen
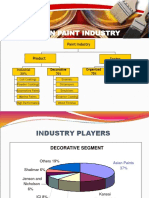
- Market Study of Paint IndustryDokument9 SeitenMarket Study of Paint IndustryJason RogersNoch keine Bewertungen
- Powder CoatingDokument36 SeitenPowder CoatingJason Rogers100% (1)
- Mohammad Mohiuddin: What'S The Balance On My Card?Dokument3 SeitenMohammad Mohiuddin: What'S The Balance On My Card?Jason RogersNoch keine Bewertungen
- Automotive Paint Michael OlveraDokument7 SeitenAutomotive Paint Michael OlveraJason RogersNoch keine Bewertungen
- Care-Reimbursement Claim FormDokument11 SeitenCare-Reimbursement Claim FormJason RogersNoch keine Bewertungen
- HYD JD Lead Vehicle DesignerDokument2 SeitenHYD JD Lead Vehicle DesignerJason RogersNoch keine Bewertungen
- Application Note: Antenna Fundamentals: DiscussionDokument4 SeitenApplication Note: Antenna Fundamentals: DiscussioncorsairsanNoch keine Bewertungen
- Bank ChequeDokument1 SeiteBank ChequeJason RogersNoch keine Bewertungen
- Wajdi A. S. Khamayseh CV: Objectives and Resume SummaryDokument5 SeitenWajdi A. S. Khamayseh CV: Objectives and Resume SummaryJason RogersNoch keine Bewertungen
- Workholding 1 321methodDokument31 SeitenWorkholding 1 321methodJason RogersNoch keine Bewertungen
- Tool TestDokument2 SeitenTool TestJason RogersNoch keine Bewertungen
- Clip Tower Cut OutsDokument1 SeiteClip Tower Cut OutsJason RogersNoch keine Bewertungen
- Sae J902a 1967Dokument5 SeitenSae J902a 1967Jason RogersNoch keine Bewertungen
- Parallel ArchitecturesDokument56 SeitenParallel ArchitectureskalscribNoch keine Bewertungen
- Sae J287 1988 PDFDokument50 SeitenSae J287 1988 PDFJason Rogers100% (2)
- By Authority of Legally Binding Document: The United States of AmericaDokument10 SeitenBy Authority of Legally Binding Document: The United States of AmericaJason RogersNoch keine Bewertungen
- Sae J449a 1963Dokument4 SeitenSae J449a 1963Jason RogersNoch keine Bewertungen
- Designing Plastic Components - QMRplasticsDokument10 SeitenDesigning Plastic Components - QMRplasticsClara PereiraNoch keine Bewertungen
- Transmission 240509Dokument25 SeitenTransmission 240509Jason RogersNoch keine Bewertungen
- Plants Can Do MathDokument24 SeitenPlants Can Do MathkrltuNoch keine Bewertungen
- 2015 - June 2BR QP PDFDokument20 Seiten2015 - June 2BR QP PDFSimilar12345Noch keine Bewertungen
- 231-2 Biology Pp2 Marking SchemeDokument4 Seiten231-2 Biology Pp2 Marking Schemegabrielsuva6Noch keine Bewertungen
- Potential Attractions of Mangrove Ecotou B1863a04Dokument16 SeitenPotential Attractions of Mangrove Ecotou B1863a04kozuki OdenNoch keine Bewertungen
- General Surgery Exam Syllabus BlueprintDokument59 SeitenGeneral Surgery Exam Syllabus BlueprintSamiaNazNoch keine Bewertungen
- Volker Scheid ArticleDokument29 SeitenVolker Scheid ArticlethienykissNoch keine Bewertungen
- Spirulina and ChlorellaDokument5 SeitenSpirulina and Chlorellalukasz27rNoch keine Bewertungen
- Human Body Systems ProjectDokument9 SeitenHuman Body Systems Projectapi-347122933Noch keine Bewertungen
- Transcript of PBS Frontline-Inside The Teenage BrainDokument28 SeitenTranscript of PBS Frontline-Inside The Teenage Brainbrub fishNoch keine Bewertungen
- Concept of Shad Garbhakara Bhavas in Ayurveda: A Review ArticleDokument2 SeitenConcept of Shad Garbhakara Bhavas in Ayurveda: A Review Articlesrikanth PosaNoch keine Bewertungen
- 10.1 MeiosisDokument38 Seiten10.1 Meiosismike bevnNoch keine Bewertungen
- 3rd Week of Development EmbryologyDokument90 Seiten3rd Week of Development EmbryologySomeoneNoch keine Bewertungen
- PigmentosDokument22 SeitenPigmentosEdgarLoman3Noch keine Bewertungen
- MEGA: A Biologist-Centric Software For Evolutionary Analysis of DNA and Protein SequencesDokument8 SeitenMEGA: A Biologist-Centric Software For Evolutionary Analysis of DNA and Protein SequencesJavier VázquezNoch keine Bewertungen
- 11 Jirr 011 Jose JackfruitDokument14 Seiten11 Jirr 011 Jose Jackfruitaulia dyasti maurendaNoch keine Bewertungen
- MCQ For Oral SurgeryDokument9 SeitenMCQ For Oral Surgeryعلي رؤوف جسام عبيدNoch keine Bewertungen
- Complete Blood Picture: 60 Year Female 23321506381Dokument3 SeitenComplete Blood Picture: 60 Year Female 23321506381SilavioNoch keine Bewertungen
- Narrow Band ApproachDokument3 SeitenNarrow Band ApproachRamsha Shahid100% (1)
- Nevada Sagebrush Archives 03/05/13Dokument16 SeitenNevada Sagebrush Archives 03/05/13The Nevada SagebrushNoch keine Bewertungen
- Are You Trying To Get Some - Are You Truly Willing To Go All in - Daily StormerDokument8 SeitenAre You Trying To Get Some - Are You Truly Willing To Go All in - Daily Stormerk_m_4000Noch keine Bewertungen
- Genetic Engineering Speech OutlineDokument2 SeitenGenetic Engineering Speech OutlineAneesh MalhotraNoch keine Bewertungen
- advtJRF DIPAS212023Dokument4 SeitenadvtJRF DIPAS212023Rathod Chandra SekharNoch keine Bewertungen
- Book of AbstractsDokument224 SeitenBook of AbstractsSasa RudanNoch keine Bewertungen