Das könnte Ihnen auch gefallen
- Fat Reduction. Pathophysiology and Treatment Strategies (Liposuction)Dokument13 SeitenFat Reduction. Pathophysiology and Treatment Strategies (Liposuction)Anonymous LnWIBo1GNoch keine Bewertungen
- Understanding Thread Lifting (History)Dokument5 SeitenUnderstanding Thread Lifting (History)Anonymous LnWIBo1G100% (1)
- The Evolution of Mastectomy Surgical Technique - From Mutilation To MedicineDokument8 SeitenThe Evolution of Mastectomy Surgical Technique - From Mutilation To MedicineAnonymous LnWIBo1GNoch keine Bewertungen
- Surgical Techniques in Breast ConservationDokument6 SeitenSurgical Techniques in Breast ConservationAnonymous LnWIBo1GNoch keine Bewertungen
- Trends and Evolution of Thread Lifting - PDO Vs PLLA Vs PCL (Type)Dokument6 SeitenTrends and Evolution of Thread Lifting - PDO Vs PLLA Vs PCL (Type)Anonymous LnWIBo1G100% (1)
- A Practical Precaution Relevant To Facial Injections (Reply)Dokument1 SeiteA Practical Precaution Relevant To Facial Injections (Reply)Anonymous LnWIBo1GNoch keine Bewertungen
- Transcutaneous Lower Blepharoplasty With Canthopexy When IndicatedDokument7 SeitenTranscutaneous Lower Blepharoplasty With Canthopexy When IndicatedAnonymous LnWIBo1GNoch keine Bewertungen
- A Journey Through Liposuction and Liposculture - Review (2017)Dokument8 SeitenA Journey Through Liposuction and Liposculture - Review (2017)Anonymous LnWIBo1GNoch keine Bewertungen
- The Effects of Platelet-Rich Plasma On Healing of Partial Thickness Burns in A Porcine ModelDokument8 SeitenThe Effects of Platelet-Rich Plasma On Healing of Partial Thickness Burns in A Porcine ModelAnonymous LnWIBo1GNoch keine Bewertungen
- A Practical Precaution Relevant To Facial InjectionsDokument1 SeiteA Practical Precaution Relevant To Facial InjectionsAnonymous LnWIBo1GNoch keine Bewertungen
- Lower Eyelid Blepharoplasty With Lateral Canthal SupportDokument7 SeitenLower Eyelid Blepharoplasty With Lateral Canthal SupportAnonymous LnWIBo1GNoch keine Bewertungen
- Reverse Anterolateral Thigh Flap To Revise A Below-Knee Amputation Stump at The Mid-Tibial Level PDFDokument4 SeitenReverse Anterolateral Thigh Flap To Revise A Below-Knee Amputation Stump at The Mid-Tibial Level PDFAnonymous LnWIBo1GNoch keine Bewertungen
- Managing Lower Eyelid Malposition After BlepharoplastyDokument3 SeitenManaging Lower Eyelid Malposition After BlepharoplastyAnonymous LnWIBo1GNoch keine Bewertungen
- Lower Eyelid Blepharoplasty With Lateral Canthal SupportDokument7 SeitenLower Eyelid Blepharoplasty With Lateral Canthal SupportAnonymous LnWIBo1GNoch keine Bewertungen
- Complications of Thread Lift and How To Manage - Thread Protrusion, Infection, Dimpling and BruisingDokument4 SeitenComplications of Thread Lift and How To Manage - Thread Protrusion, Infection, Dimpling and BruisingAnonymous LnWIBo1G0% (1)
- Short Incisional Double-Eyelid Blepharoplasty For Asian PatientsDokument7 SeitenShort Incisional Double-Eyelid Blepharoplasty For Asian PatientsAnonymous LnWIBo1GNoch keine Bewertungen
- A Method of Internal Splinting For Unstable Nasal FracturesDokument7 SeitenA Method of Internal Splinting For Unstable Nasal FracturesAnonymous LnWIBo1GNoch keine Bewertungen
- Asian Blepharoplasty - Ageing Patterns, Anatomophysiological Considerations and Ethnic DifferencesDokument6 SeitenAsian Blepharoplasty - Ageing Patterns, Anatomophysiological Considerations and Ethnic DifferencesAnonymous LnWIBo1GNoch keine Bewertungen
- The Society For Vascular Surgery: Clinical Practice Guidelines For The Surgical Placement and Maintenance of Arteriovenous Hemodialysis AccessDokument24 SeitenThe Society For Vascular Surgery: Clinical Practice Guidelines For The Surgical Placement and Maintenance of Arteriovenous Hemodialysis AccessAnonymous LnWIBo1GNoch keine Bewertungen
- Suspension Technique For Unstable Nasal Bones (Fracture)Dokument2 SeitenSuspension Technique For Unstable Nasal Bones (Fracture)Anonymous LnWIBo1GNoch keine Bewertungen
- Fat Grafting To The Forehead-Glabella-Radix Complex and Pyriform Aperture - Aesthetic and Anti-Aging ImplicationsDokument11 SeitenFat Grafting To The Forehead-Glabella-Radix Complex and Pyriform Aperture - Aesthetic and Anti-Aging ImplicationsAnonymous LnWIBo1GNoch keine Bewertungen
- Reverse Anterolateral Thigh Flap To Revise A Below-Knee Amputation Stump at The Mid-Tibial Level PDFDokument4 SeitenReverse Anterolateral Thigh Flap To Revise A Below-Knee Amputation Stump at The Mid-Tibial Level PDFAnonymous LnWIBo1GNoch keine Bewertungen
- Aesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinDokument7 SeitenAesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinAnonymous LnWIBo1GNoch keine Bewertungen
- Classification and Application of The Distally-Based Thigh Flap PDFDokument8 SeitenClassification and Application of The Distally-Based Thigh Flap PDFAnonymous LnWIBo1GNoch keine Bewertungen
- Efficacy of External Fixation Following Nasal Manipulation Under Local Anaesthesia PDFDokument5 SeitenEfficacy of External Fixation Following Nasal Manipulation Under Local Anaesthesia PDFAnonymous LnWIBo1GNoch keine Bewertungen
- Primary and Staged Transposition Arteriovenous Fistulas (Superficialization)Dokument5 SeitenPrimary and Staged Transposition Arteriovenous Fistulas (Superficialization)Anonymous LnWIBo1GNoch keine Bewertungen
- Efficacy of External Fixation Following Nasal Manipulation Under Local Anaesthesia PDFDokument5 SeitenEfficacy of External Fixation Following Nasal Manipulation Under Local Anaesthesia PDFAnonymous LnWIBo1GNoch keine Bewertungen
- Bitumen Burn First AidDokument2 SeitenBitumen Burn First AidAnonymous LnWIBo1GNoch keine Bewertungen
- The Current Practice of The Management of Little Finger Metacarpal Fractures... (2012)Dokument10 SeitenThe Current Practice of The Management of Little Finger Metacarpal Fractures... (2012)Anonymous LnWIBo1GNoch keine Bewertungen
- Understanding Thread Lifting (History)Dokument5 SeitenUnderstanding Thread Lifting (History)Anonymous LnWIBo1G100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Health Unit LP - Days 1-5Dokument16 SeitenHealth Unit LP - Days 1-5api-568715148Noch keine Bewertungen
- QRA BOOKLET GUIDANCEDokument37 SeitenQRA BOOKLET GUIDANCETatjana BrankovićNoch keine Bewertungen
- Capstone Project FinalDokument16 SeitenCapstone Project Finalapi-409052955Noch keine Bewertungen
- Anticipatory GuidanceDokument37 SeitenAnticipatory GuidanceSnap18Noch keine Bewertungen
- Mechanical and Chemical Plaque ControlDokument59 SeitenMechanical and Chemical Plaque ControlJyotica Jos75% (4)
- Music and Arts QuizDokument6 SeitenMusic and Arts QuizTino SalabsabNoch keine Bewertungen
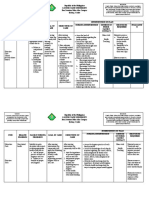
- Cavite State University Nursing Intervention for Hypertension ManagementDokument4 SeitenCavite State University Nursing Intervention for Hypertension Managementteuuuu100% (1)
- Management and Prevention of Gingival Recession. Merijohn-2016-Periodontology - 2000 Bogdan Chiriac GR 9Dokument15 SeitenManagement and Prevention of Gingival Recession. Merijohn-2016-Periodontology - 2000 Bogdan Chiriac GR 9camelia_ioana_14100% (1)
- A Study On Customer Satisfaction Towards Colgate Toothpaste With Reference To Omalur TownDokument6 SeitenA Study On Customer Satisfaction Towards Colgate Toothpaste With Reference To Omalur TownManikanta ShaasthaNoch keine Bewertungen
- Debra Poneman Secrets For Lifelong RadianceDokument16 SeitenDebra Poneman Secrets For Lifelong RadianceThiago GueirosNoch keine Bewertungen
- Yash PaulDokument8 SeitenYash Paulal rzNoch keine Bewertungen
- Oral and Dental HealthDokument21 SeitenOral and Dental HealthMaricor OnateNoch keine Bewertungen
- ContentServer Asp-6Dokument5 SeitenContentServer Asp-6Estaf EmkeyzNoch keine Bewertungen
- Buku Informasi Kandungan Gizi PJASDokument6 SeitenBuku Informasi Kandungan Gizi PJASRelinda PriharumNoch keine Bewertungen
- Group 1 Sec B Cottle IndiaDokument9 SeitenGroup 1 Sec B Cottle Indiasujeet palNoch keine Bewertungen
- The Huddle 5-18-15 EDITDokument4 SeitenThe Huddle 5-18-15 EDITSarah DoyleNoch keine Bewertungen
- Pepsodent Tooth PasteDokument40 SeitenPepsodent Tooth PasteKing Nitin AgnihotriNoch keine Bewertungen
- Fixed Orthodontic Retainers: A ReviewDokument5 SeitenFixed Orthodontic Retainers: A ReviewhelmysiswantoNoch keine Bewertungen
- Oral Hygiene TechniquesDokument2 SeitenOral Hygiene TechniquesDredd Alejo Sumbad100% (1)
- Сlinical case 1:: 1. What can be used for diagnosis of hard tooth tissue pathology of teeth 1.1, 1.2, 1.3, 2.1, 2.2, 2.3Dokument15 SeitenСlinical case 1:: 1. What can be used for diagnosis of hard tooth tissue pathology of teeth 1.1, 1.2, 1.3, 2.1, 2.2, 2.3Mouna Jomaa DhifaouiNoch keine Bewertungen
- GE Elect 3 Module 4 5Dokument9 SeitenGE Elect 3 Module 4 5Princess AndreaNoch keine Bewertungen
- Hha ExamDokument8 SeitenHha ExamOlaya alghareniNoch keine Bewertungen
- Original Research: Jurnal Berkala EpidemiologiDokument8 SeitenOriginal Research: Jurnal Berkala EpidemiologiTataNoch keine Bewertungen
- UAE Health System & Daman Insurance A Thesis Submitted To Sarhad UniversityDokument69 SeitenUAE Health System & Daman Insurance A Thesis Submitted To Sarhad UniversityawaisNoch keine Bewertungen
- Marketing Mix and Strategies of Colgate Palmolive India LtdDokument18 SeitenMarketing Mix and Strategies of Colgate Palmolive India Ltdgunjan100Noch keine Bewertungen
- Davis 2014Dokument11 SeitenDavis 2014Monica JohanaNoch keine Bewertungen
- Community Dentistry Final Questions From Board Review Flashcards - QuizletDokument5 SeitenCommunity Dentistry Final Questions From Board Review Flashcards - QuizletRMNoch keine Bewertungen
- Public HealthDokument131 SeitenPublic Healthmzk_dds100% (2)
- DR Seuss - The Tooth Book - ENDokument15 SeitenDR Seuss - The Tooth Book - ENLovely OwensNoch keine Bewertungen
- Vestige Product Price List 2018Dokument4 SeitenVestige Product Price List 2018Vicky KatariaNoch keine Bewertungen