Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Benchmade v. HogueDokument13 SeitenBenchmade v. HoguePortland Business JournalNoch keine Bewertungen
- Class and Collective Action Allegation Complaint-Dkt 1Dokument43 SeitenClass and Collective Action Allegation Complaint-Dkt 1Portland Business JournalNoch keine Bewertungen
- 2020 BizWomen BioBook - 021320Dokument14 Seiten2020 BizWomen BioBook - 021320Portland Business JournalNoch keine Bewertungen
- ComplaintDokument14 SeitenComplaintPortland Business JournalNoch keine Bewertungen
- USA v. Gatto Opening StatementsDokument87 SeitenUSA v. Gatto Opening StatementsPortland Business JournalNoch keine Bewertungen
- Lawsuit Filed To Stop Portland From Allowing Homeless CampsDokument15 SeitenLawsuit Filed To Stop Portland From Allowing Homeless CampsPortland Business JournalNoch keine Bewertungen
- Seaport Airlines Reorganization PlanDokument75 SeitenSeaport Airlines Reorganization PlanPortland Business JournalNoch keine Bewertungen
- PPSs Response To Letter of Intent Fro M Macadam Forbes - Final - April 27Dokument1 SeitePPSs Response To Letter of Intent Fro M Macadam Forbes - Final - April 27Portland Business JournalNoch keine Bewertungen
- Appendix 1: List of Potentially Regulated Entities: Fossil Fuel SuppliersDokument5 SeitenAppendix 1: List of Potentially Regulated Entities: Fossil Fuel SuppliersPortland Business JournalNoch keine Bewertungen
- Ertischek V ViewpointDokument23 SeitenErtischek V ViewpointPortland Business JournalNoch keine Bewertungen
- Intel Memo To EmployeesDokument3 SeitenIntel Memo To EmployeesPortland Business JournalNoch keine Bewertungen
- Letter From Oracle To Sec. BurwellDokument47 SeitenLetter From Oracle To Sec. BurwellPortland Business JournalNoch keine Bewertungen
- SEC Aequitas ComplaintDokument30 SeitenSEC Aequitas ComplaintPortland Business JournalNoch keine Bewertungen
- Health Republic's U.S. SuitDokument25 SeitenHealth Republic's U.S. SuitPortland Business JournalNoch keine Bewertungen
- Oracle Injunction Over Kitzhaber EmailsDokument27 SeitenOracle Injunction Over Kitzhaber EmailsPortland Business JournalNoch keine Bewertungen
- NuScale Power CEO Elected Vice Chairman of U.S. Chamber of CommerceDokument2 SeitenNuScale Power CEO Elected Vice Chairman of U.S. Chamber of CommercePortland Business JournalNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Iso 15011-2-2009Dokument26 SeitenIso 15011-2-2009marcosNoch keine Bewertungen
- Work of Asha Bhavan Centre - A Nonprofit Indian Organisation For Persons With DisabilityDokument10 SeitenWork of Asha Bhavan Centre - A Nonprofit Indian Organisation For Persons With DisabilityAsha Bhavan CentreNoch keine Bewertungen
- Margarita ForesDokument20 SeitenMargarita ForesKlarisse YoungNoch keine Bewertungen
- Allison Weech Final ResumeDokument1 SeiteAllison Weech Final Resumeapi-506177291Noch keine Bewertungen
- Speaking Topics For Final ReviewDokument3 SeitenSpeaking Topics For Final ReviewNhư ÝNoch keine Bewertungen
- URICA TestDokument3 SeitenURICA TestCristy PagalanNoch keine Bewertungen
- Plasma Arc Machining (Pam) : Mechanical Engineering Department I.I.T Guwahati-781039 E-Mail: Manasdas@iitg - Ernet.inDokument15 SeitenPlasma Arc Machining (Pam) : Mechanical Engineering Department I.I.T Guwahati-781039 E-Mail: Manasdas@iitg - Ernet.inSrinivasanNoch keine Bewertungen
- Hema Lec HematopoiesisDokument8 SeitenHema Lec HematopoiesisWayne ErumaNoch keine Bewertungen
- Lab CompilationDokument11 SeitenLab CompilationJanita SiddiquiNoch keine Bewertungen
- Trillanes V PimentelDokument2 SeitenTrillanes V PimentelKirk LabowskiNoch keine Bewertungen
- AACO 7th Aviation Fuel Forum: AttendanceDokument3 SeitenAACO 7th Aviation Fuel Forum: AttendanceJigisha Vasa0% (1)
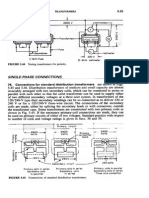
- Transformers ConnectionsDokument6 SeitenTransformers Connectionsgeorgel1980Noch keine Bewertungen
- UBKV Ranking Proforma With Annexures 2018 PDFDokument53 SeitenUBKV Ranking Proforma With Annexures 2018 PDFSubinay Saha RoyNoch keine Bewertungen
- Unit Two The Health Benefits of Physical ActivityDokument10 SeitenUnit Two The Health Benefits of Physical ActivityYoseph DefaruNoch keine Bewertungen
- What Does She/He Look Like?: Height Build AGEDokument18 SeitenWhat Does She/He Look Like?: Height Build AGEHenrich Garcia LimaNoch keine Bewertungen
- Factors That Contribute To Successful BakingDokument8 SeitenFactors That Contribute To Successful BakingErrol San Juan100% (1)
- Celltac MEK 6500Dokument3 SeitenCelltac MEK 6500RiduanNoch keine Bewertungen
- Carbo Hi DratDokument11 SeitenCarbo Hi DratILHAM BAGUS DARMA .NNoch keine Bewertungen
- Child Case History FDokument6 SeitenChild Case History FSubhas RoyNoch keine Bewertungen
- Sociology/Marriage PresentationDokument31 SeitenSociology/Marriage PresentationDoofSadNoch keine Bewertungen
- Sampoong Department Store - A Literary Critique (Mimetic Theory)Dokument2 SeitenSampoong Department Store - A Literary Critique (Mimetic Theory)Ron Marc CaneteNoch keine Bewertungen
- Meditran SX Sae 15w 40 API CH 4Dokument1 SeiteMeditran SX Sae 15w 40 API CH 4Aam HudsonNoch keine Bewertungen
- Starters Flash CardsDokument28 SeitenStarters Flash CardsNara GarridoNoch keine Bewertungen
- Rate Break Up 15500Dokument1 SeiteRate Break Up 15500Yash Raj Bhardwaj100% (1)
- A656 GR 80 Brochure 06-26-08Dokument2 SeitenA656 GR 80 Brochure 06-26-08OsmanNoch keine Bewertungen
- The Mental MeltdownDokument5 SeitenThe Mental Meltdownapi-460020991Noch keine Bewertungen
- Governance StructureDokument1 SeiteGovernance StructureJoydip MukhopadhyayNoch keine Bewertungen
- Lesson 4: Health and Fitness AdvertisingDokument4 SeitenLesson 4: Health and Fitness AdvertisingCatherineNoch keine Bewertungen
- Material: Safety Data SheetDokument3 SeitenMaterial: Safety Data SheetMichael JoudalNoch keine Bewertungen
- Biology Project Cronary Heart Diseas (CHD)Dokument7 SeitenBiology Project Cronary Heart Diseas (CHD)احمد المغربي50% (2)