Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- 30 Clinical Cases From EmedicineDokument103 Seiten30 Clinical Cases From EmedicineBahi Alastal100% (3)
- 2 A 19 B 3 ResearchDokument43 Seiten2 A 19 B 3 ResearchalaaNoch keine Bewertungen
- Registration Form 20140403Dokument2 SeitenRegistration Form 20140403alaaNoch keine Bewertungen
- Diabetes 2008 Pereira 56 63Dokument8 SeitenDiabetes 2008 Pereira 56 63alaaNoch keine Bewertungen
- 100 Commonly Tested Facts For MRCP Part 1Dokument5 Seiten100 Commonly Tested Facts For MRCP Part 1Khalid AbdelazizNoch keine Bewertungen
- Diabetes 2015 Ahrén 715 7Dokument3 SeitenDiabetes 2015 Ahrén 715 7alaaNoch keine Bewertungen
- ModyDokument8 SeitenModyFarah Soraya EffendiNoch keine Bewertungen
- 2010 Revised Criteria Classification RaDokument13 Seiten2010 Revised Criteria Classification RaFarhan MuhammadNoch keine Bewertungen
- 209215Dokument10 Seiten209215alaaNoch keine Bewertungen
- VHRM 8216 Type 2 Diabetes Postprandial Hyperglycemia and Cardiovascul 030510Dokument11 SeitenVHRM 8216 Type 2 Diabetes Postprandial Hyperglycemia and Cardiovascul 030510alaaNoch keine Bewertungen
- TCRM 39564 Therapeutic Interventions To Reduce The Risk of Progression 032014Dokument16 SeitenTCRM 39564 Therapeutic Interventions To Reduce The Risk of Progression 032014alaaNoch keine Bewertungen
- Selected ReadingsDokument26 SeitenSelected ReadingsalaaNoch keine Bewertungen
- Dual Release HydrocortisoneDokument9 SeitenDual Release HydrocortisonealaaNoch keine Bewertungen
- TCRM 39564 Therapeutic Interventions To Reduce The Risk of Progression 032014Dokument16 SeitenTCRM 39564 Therapeutic Interventions To Reduce The Risk of Progression 032014alaaNoch keine Bewertungen
- Anticoagulation in Atrial Fibrillation: ChadsDokument1 SeiteAnticoagulation in Atrial Fibrillation: ChadsalaaNoch keine Bewertungen
- CIA-Marouf-2009-4-187-190-INSULIN ASPART-3142Dokument4 SeitenCIA-Marouf-2009-4-187-190-INSULIN ASPART-3142alaaNoch keine Bewertungen
- 62 FullDokument12 Seiten62 FullalaaNoch keine Bewertungen
- BP Measurement ChecklistDokument1 SeiteBP Measurement ChecklistBeatrice ChiaNoch keine Bewertungen
- Circulation 2015 Baddour 1435 86Dokument54 SeitenCirculation 2015 Baddour 1435 86alaaNoch keine Bewertungen
- Ethics Handbook For ResidentsDokument254 SeitenEthics Handbook For Residentsalaa100% (6)
- GerdDokument60 SeitenGerdalaaNoch keine Bewertungen
- Age of Transfused Blood in Critically Ill Adults PDFDokument9 SeitenAge of Transfused Blood in Critically Ill Adults PDFdrhwek2001Noch keine Bewertungen
- RCP Consultant Physicians Working With PatientsDokument266 SeitenRCP Consultant Physicians Working With PatientsalaaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- GO Health Information StopDokument2 SeitenGO Health Information StopNixZ Teruel2Noch keine Bewertungen
- Record Below The Total Number of Cases and Deaths For Each Disease/condition For The Current WeekDokument2 SeitenRecord Below The Total Number of Cases and Deaths For Each Disease/condition For The Current WeekYohannes MengistNoch keine Bewertungen
- Microbiology and Parasitology HandoutsDokument5 SeitenMicrobiology and Parasitology HandoutsJudy BaguiwenNoch keine Bewertungen
- Pulmonology Techniques Breakthrough by Slidesgo 2Dokument33 SeitenPulmonology Techniques Breakthrough by Slidesgo 2BEATRIZ MACEDO VALADÃONoch keine Bewertungen
- Host ModulationDokument17 SeitenHost ModulationIbrar HumayunNoch keine Bewertungen
- Alopecia AreataDokument12 SeitenAlopecia AreataJohnNoch keine Bewertungen
- Kaqun Studies Book 2013 PDFDokument183 SeitenKaqun Studies Book 2013 PDFVeres András100% (2)
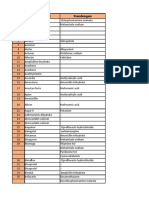
- Generic MedicinesDokument16 SeitenGeneric MedicinesAnn Christine C. ChuaNoch keine Bewertungen
- DESIGN AND DEVELOPMENT OF C-ARM MACHINE - Pptx.feem - Backup - 265248Dokument11 SeitenDESIGN AND DEVELOPMENT OF C-ARM MACHINE - Pptx.feem - Backup - 265248TamilandaNoch keine Bewertungen
- DPL OperationDokument2 SeitenDPL OperationTao JunNoch keine Bewertungen
- Gestational DiabetesDokument42 SeitenGestational Diabetesjohn jumborock100% (1)
- Analgesic Policy (2009)Dokument84 SeitenAnalgesic Policy (2009)Ramon MagsaysayNoch keine Bewertungen
- NCP AnxietyDokument1 SeiteNCP AnxietyUnang MagnayeNoch keine Bewertungen
- Velez College Cebu City, Philippines: GEC - PC GEC - MMW Pmls 1Dokument3 SeitenVelez College Cebu City, Philippines: GEC - PC GEC - MMW Pmls 1Armyl Raul CanadaNoch keine Bewertungen
- Factors in The Relationship Between Epilepsy and Behavioral DisordersDokument19 SeitenFactors in The Relationship Between Epilepsy and Behavioral DisordersEdya YopiNoch keine Bewertungen
- Clikstar Dispositivo Administrador InsulinaDokument11 SeitenClikstar Dispositivo Administrador InsulinaHenry SilvaNoch keine Bewertungen
- ISBTABS 369 Preview 6Dokument1 SeiteISBTABS 369 Preview 6arfat lusinantoNoch keine Bewertungen
- Drug StudyDokument25 SeitenDrug StudyshakiraNoch keine Bewertungen
- 04 Vital Signs AssesmentDokument20 Seiten04 Vital Signs AssesmentChristine SangilNoch keine Bewertungen
- Use of "Zingiber Officinale Roscoe L" Root in Various DiseasesDokument8 SeitenUse of "Zingiber Officinale Roscoe L" Root in Various DiseasesCentral Asian StudiesNoch keine Bewertungen
- Four Phases of Intravenous Fluid Therapy A Conceptual Model British Journal of Anaesthesia 2014Dokument8 SeitenFour Phases of Intravenous Fluid Therapy A Conceptual Model British Journal of Anaesthesia 2014Antonia Holguin HoyosNoch keine Bewertungen
- Penatalaksanaan DemamDokument39 SeitenPenatalaksanaan DemamClaraRotendownNoch keine Bewertungen
- Healthcare ProfessionalismDokument28 SeitenHealthcare ProfessionalismAnjo CincoNoch keine Bewertungen
- Tugas Obat KerasDokument34 SeitenTugas Obat KerasaminnatuljannahNoch keine Bewertungen
- Larynx, Trachea, Lung and PleuraDokument60 SeitenLarynx, Trachea, Lung and PleuraKatNoch keine Bewertungen
- Teaching Students With Autism Spectrum DisordersDokument155 SeitenTeaching Students With Autism Spectrum DisordersAnonymous Pj6Odj0% (1)
- ORS Program Book 2015 WebDokument164 SeitenORS Program Book 2015 Webaiakoby100% (1)
- Homeopathy How Do Homeopathic Remedies Work - Hormesis - Pheromones - Spiritual - Energy Plane - HomeopatDokument1 SeiteHomeopathy How Do Homeopathic Remedies Work - Hormesis - Pheromones - Spiritual - Energy Plane - HomeopatnaveenNoch keine Bewertungen
- Manuscript of Step 2 CsDokument8 SeitenManuscript of Step 2 CsJason SteelNoch keine Bewertungen