Das könnte Ihnen auch gefallen
- Respuestas 1-8 BDokument1 SeiteRespuestas 1-8 BRuben R Cardona75% (8)
- PEBC Application Pharmacist Document EvaluationDokument2 SeitenPEBC Application Pharmacist Document EvaluationmcarthooNoch keine Bewertungen
- Naplex Mpje Bulletin May 14 2018Dokument50 SeitenNaplex Mpje Bulletin May 14 2018Clayton JensenNoch keine Bewertungen
- Reference Guide For Foreign Pharmacy Licensing ExamDokument6 SeitenReference Guide For Foreign Pharmacy Licensing Examcarp liciniaNoch keine Bewertungen
- Refer Books Sort ListDokument12 SeitenRefer Books Sort ListDr-Ram ChowdharyNoch keine Bewertungen
- Naplex Pass Rates 2013Dokument5 SeitenNaplex Pass Rates 2013amzeidanNoch keine Bewertungen
- Pebc Evaluating Exam Sample QuestionDokument50 SeitenPebc Evaluating Exam Sample QuestionZain zanzoonNoch keine Bewertungen
- SHARGELDokument2.115 SeitenSHARGELFrançoise BNoch keine Bewertungen
- Epp5 Fall 2020 The Practice of Pharmacy in Florida - Laws Rules - Alvarez Student Version 3 SlidesDokument25 SeitenEpp5 Fall 2020 The Practice of Pharmacy in Florida - Laws Rules - Alvarez Student Version 3 Slidesapi-552486649Noch keine Bewertungen
- 58 Drug Information ResourcesDokument2 Seiten58 Drug Information Resourcesagent2catNoch keine Bewertungen
- Studying RoutineDokument12 SeitenStudying RoutineKelvin Lim Wei Liang100% (1)
- Foreign Grads Info LetterDokument3 SeitenForeign Grads Info LetterRoman WinerNoch keine Bewertungen
- Senior Pharmacist: Passbooks Study GuideVon EverandSenior Pharmacist: Passbooks Study GuideNoch keine Bewertungen
- FPGEC Application Bulletin 06-02-17Dokument48 SeitenFPGEC Application Bulletin 06-02-17Debjani BaidyaNoch keine Bewertungen
- FPGEC ApplicationBulletin 2019Dokument44 SeitenFPGEC ApplicationBulletin 2019espharma educationNoch keine Bewertungen
- FPGEEDokument1 SeiteFPGEERushank ShuklaNoch keine Bewertungen
- Naplex Mpje: 2017 Candidate Registration BulletinDokument51 SeitenNaplex Mpje: 2017 Candidate Registration BulletinLam LamNoch keine Bewertungen
- Complete Fpgee Application SummaryDokument6 SeitenComplete Fpgee Application SummaryStephanie Camille Samonte100% (1)
- Pharmacy Historypharmacopoeia 180817063405 PDFDokument111 SeitenPharmacy Historypharmacopoeia 180817063405 PDFchandra sekhar gowra0% (1)
- Coursera - Pharmacist Licensure ProcsDokument13 SeitenCoursera - Pharmacist Licensure Procsaudio habibiNoch keine Bewertungen
- Naplex Mpje BulletinDokument49 SeitenNaplex Mpje BulletinAssignment Abroad0% (1)
- Corrections - The APhA Complete Review For The FPGEEDokument2 SeitenCorrections - The APhA Complete Review For The FPGEEBlsNoch keine Bewertungen
- Careers in PharmacyDokument6 SeitenCareers in PharmacyChaitanya GaddeNoch keine Bewertungen
- UofMd School of Pharmacy CatalogDokument95 SeitenUofMd School of Pharmacy CatalogjolihooNoch keine Bewertungen
- PEBC EnglishDokument4 SeitenPEBC EnglishSaiKai54Noch keine Bewertungen
- Fpgee PlanDokument9 SeitenFpgee PlanDoha AnberNoch keine Bewertungen
- Euler MathematicsDokument36 SeitenEuler MathematicsJohn HamiltonNoch keine Bewertungen
- Gateway:: The Fee For Enrolment in The Gateway Is $340Dokument5 SeitenGateway:: The Fee For Enrolment in The Gateway Is $340Farhan aliNoch keine Bewertungen
- PEBC Application InstructionsDokument3 SeitenPEBC Application InstructionsParthNoch keine Bewertungen
- PEBC Application Pharmacist Document EvaluationDokument2 SeitenPEBC Application Pharmacist Document EvaluationCindy Rose MisenaNoch keine Bewertungen
- Fpgec Certification: FpgeeDokument43 SeitenFpgec Certification: FpgeeSana KhanNoch keine Bewertungen
- Mock TestDokument20 SeitenMock Testironcahir61100% (1)
- NAPLEX Pass Rates 2016 2017 and 2018Dokument14 SeitenNAPLEX Pass Rates 2016 2017 and 2018Lorena CalderonNoch keine Bewertungen
- CLEAR 2005 - Scores and Reports3 - CObyrneLilaDokument21 SeitenCLEAR 2005 - Scores and Reports3 - CObyrneLilaMithNoch keine Bewertungen
- Pebc Document Evaluation FormDokument18 SeitenPebc Document Evaluation FormMonika Bluesky OverseasNoch keine Bewertungen
- 2015 2016 College of Pharmacy Student HandbookDokument62 Seiten2015 2016 College of Pharmacy Student HandbookFiya AwanNoch keine Bewertungen
- Guidelines Minimum Standard Pharmacies HospitalsDokument11 SeitenGuidelines Minimum Standard Pharmacies HospitalsEngyKamalNoch keine Bewertungen
- PEBCHandbookDokument15 SeitenPEBCHandbookversion1403Noch keine Bewertungen
- Top 100 Drugs in CanadaDokument25 SeitenTop 100 Drugs in CanadaMohamed Omer100% (1)
- Controlled Substances LawsDokument8 SeitenControlled Substances LawsJames Lindon100% (1)
- Part A: Job Analysis Information Sheet of Hospital PharmacistDokument3 SeitenPart A: Job Analysis Information Sheet of Hospital PharmacistTan Su SuanNoch keine Bewertungen
- FPGEC Application BulletinDokument30 SeitenFPGEC Application Bulletinshamram20Noch keine Bewertungen
- JP Refresher Seminar Useful Websites: Legislation Federal LegislationDokument27 SeitenJP Refresher Seminar Useful Websites: Legislation Federal LegislationHeba Ahmed El Nagar100% (1)
- PEBC EE BlueprintDokument2 SeitenPEBC EE BlueprintcoolchapNoch keine Bewertungen
- OSCE - Sample Chapter PDFDokument32 SeitenOSCE - Sample Chapter PDFAndrés LLanos PrietoNoch keine Bewertungen
- Pharmacist Evaluating Exam - References and Resources ListDokument4 SeitenPharmacist Evaluating Exam - References and Resources Listmahmoud jalloulNoch keine Bewertungen
- 8 B. Social, Behavioral, Economic, and Administrative SciencesDokument140 Seiten8 B. Social, Behavioral, Economic, and Administrative SciencesSamson SeiduNoch keine Bewertungen
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDokument13 SeitenAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilNoch keine Bewertungen
- First Section of Manan's TheoryDokument34 SeitenFirst Section of Manan's TheoryM Imran SajidNoch keine Bewertungen
- Naplex MpjeDokument35 SeitenNaplex MpjeAtlantis ManNoch keine Bewertungen
- CoursesDokument2 SeitenCoursesapi-586042393Noch keine Bewertungen
- Cal Pharmaspirit PH Cal Q ADokument49 SeitenCal Pharmaspirit PH Cal Q AAriadne BalmacedaNoch keine Bewertungen
- The Pharmacy Examining Board of Canada: Le Bureau Des Examinateurs en Pharmacie Du CanadaDokument2 SeitenThe Pharmacy Examining Board of Canada: Le Bureau Des Examinateurs en Pharmacie Du CanadaSylvia AmakaNoch keine Bewertungen
- Apc0271 V4 PDFDokument53 SeitenApc0271 V4 PDFDrAnisha PatelNoch keine Bewertungen
- FPGEC Application Bulletin 073013Dokument30 SeitenFPGEC Application Bulletin 073013YerimDeVeraNoch keine Bewertungen
- FPGEE Blueprint: Area 1 - Basic Biomedical Sciences - 21%Dokument12 SeitenFPGEE Blueprint: Area 1 - Basic Biomedical Sciences - 21%Raafat A. Issaq100% (2)
- PHARMACY PRACTICE & CLINICAL PHARMACY dEPARTMENT (PDFDrive) PDFDokument83 SeitenPHARMACY PRACTICE & CLINICAL PHARMACY dEPARTMENT (PDFDrive) PDFDinesh Kumar YadavNoch keine Bewertungen
- Frequently Asked Questions About Canadian Pharmacy ResidenciesDokument2 SeitenFrequently Asked Questions About Canadian Pharmacy Residencieskuber1Noch keine Bewertungen
- Lexicon of Pharmacy: A Concise up-to-date referenceVon EverandLexicon of Pharmacy: A Concise up-to-date referenceNoch keine Bewertungen
- The Art of Creative TranslationDokument2 SeitenThe Art of Creative Translationzeen tarekNoch keine Bewertungen
- KsasDokument5 SeitenKsasapi-268236603Noch keine Bewertungen
- A Template To Be Used by The Students For Typesetting Project Report or DissertationDokument18 SeitenA Template To Be Used by The Students For Typesetting Project Report or DissertationMuhammad Tanzeel Qaisar DogarNoch keine Bewertungen
- Favorite Subject of Grade 10 - ChastityDokument2 SeitenFavorite Subject of Grade 10 - ChastitySheery Mariz FernandezNoch keine Bewertungen
- Prabhnoor Kaur: E-Mail: PhoneDokument1 SeitePrabhnoor Kaur: E-Mail: Phonesukhwinder singh bediNoch keine Bewertungen
- Prepare Second Edition Level 1: List It!Dokument2 SeitenPrepare Second Edition Level 1: List It!Mar PerezNoch keine Bewertungen
- NatorpDokument1 SeiteNatorpIgnacio RojasNoch keine Bewertungen
- Lesson Plan English 10Dokument6 SeitenLesson Plan English 10Butch RejusoNoch keine Bewertungen
- Metacognition in Reading: Reviewing The Literature: Abidin Pammu, Zaini Amir, Tg. Nor Rizan Tg. Mohd. MaasumDokument22 SeitenMetacognition in Reading: Reviewing The Literature: Abidin Pammu, Zaini Amir, Tg. Nor Rizan Tg. Mohd. MaasumNajma FitriaNoch keine Bewertungen
- Ele 3 To 5 Math UkrainianDokument22 SeitenEle 3 To 5 Math UkrainianAhmed Saeid Mahmmoud OufNoch keine Bewertungen
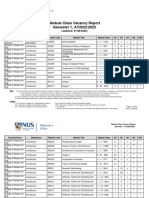
- VacancyRpt R3 2223S1Dokument273 SeitenVacancyRpt R3 2223S1Lim ShawnNoch keine Bewertungen
- Tardiness 1Dokument4 SeitenTardiness 1Ley 31Noch keine Bewertungen
- District Enhancement Training of School Heads On Instructional Leadership in The New NormalDokument7 SeitenDistrict Enhancement Training of School Heads On Instructional Leadership in The New NormalLINDO LECERANoch keine Bewertungen
- DACUM ProcessDokument72 SeitenDACUM Processjvarga.db4878Noch keine Bewertungen
- List of Als Modules 2021Dokument8 SeitenList of Als Modules 2021JULIA PoncianoNoch keine Bewertungen
- FIN4414 SyllabusDokument31 SeitenFIN4414 SyllabusQQQQQQNoch keine Bewertungen
- MeasurementDokument3 SeitenMeasurementAngelica Faye LitonjuaNoch keine Bewertungen
- Historical Foundation of EducationDokument18 SeitenHistorical Foundation of EducationJennifer Oestar100% (1)
- A. Personal InformationDokument5 SeitenA. Personal InformationInas40% (5)
- Abin Azka 10DDokument7 SeitenAbin Azka 10DAziz Tanama1Noch keine Bewertungen
- Biol 1700 - Course Outline 2019Dokument20 SeitenBiol 1700 - Course Outline 2019api-490973801Noch keine Bewertungen
- Pre TestDokument6 SeitenPre TestAngie Diño AmuraoNoch keine Bewertungen
- Mass Communication AssignmentDokument5 SeitenMass Communication AssignmentAkNoch keine Bewertungen
- Lori Obendorf Resume 2017Dokument2 SeitenLori Obendorf Resume 2017api-347145295Noch keine Bewertungen
- Narrative Report in SWTDokument13 SeitenNarrative Report in SWTQuarentai Siete LptNoch keine Bewertungen
- Esp6 - q2 - Mod7 - Paggalang Sa Suhestiyon NG KapwaDokument27 SeitenEsp6 - q2 - Mod7 - Paggalang Sa Suhestiyon NG KapwaAnna Liza B.Pantaleon100% (2)
- Discussion TextDokument2 SeitenDiscussion TextAprilia Dwi WijayantiNoch keine Bewertungen
- Dipesh - The Project ManagerDokument3 SeitenDipesh - The Project ManagerJana50% (2)
- EmpotechDokument4 SeitenEmpotechAlbern Ray BaleanNoch keine Bewertungen