Das könnte Ihnen auch gefallen
- Fenner Et Al-2015-Clinical Oral Implants ResearchDokument8 SeitenFenner Et Al-2015-Clinical Oral Implants ResearchDeyvyd LimaNoch keine Bewertungen
- Zarnadi Etal 2012Dokument6 SeitenZarnadi Etal 2012Deyvyd LimaNoch keine Bewertungen
- Dittemer Etal 2011Dokument6 SeitenDittemer Etal 2011Deyvyd LimaNoch keine Bewertungen
- Elgelke Et Al Ift 2013Dokument7 SeitenElgelke Et Al Ift 2013Deyvyd LimaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Earth Science (Metamorphic Rocks)Dokument8 SeitenEarth Science (Metamorphic Rocks)MA. ALEXIS LAURENNoch keine Bewertungen
- SAT Biochar Ethylene Poster 10 - 10b PDFDokument1 SeiteSAT Biochar Ethylene Poster 10 - 10b PDFsherifalharamNoch keine Bewertungen
- Disectie AnatomieDokument908 SeitenDisectie AnatomieMircea SimionNoch keine Bewertungen
- SPM 1449 2006 Mathematics p2 BerjawapanDokument18 SeitenSPM 1449 2006 Mathematics p2 Berjawapanpss smk selandar71% (7)
- A Presentation On-: Dr. Nikhil Oza Intern BvdumcDokument43 SeitenA Presentation On-: Dr. Nikhil Oza Intern BvdumcMaheboob GanjalNoch keine Bewertungen
- Maths All FormulasDokument5 SeitenMaths All FormulasVishnuNoch keine Bewertungen
- Earth Sciences Notes Csir-Ugc Net JRFDokument57 SeitenEarth Sciences Notes Csir-Ugc Net JRFmanas773Noch keine Bewertungen
- Listening - Homework 2: Brushes 285 RamdhanieDokument4 SeitenListening - Homework 2: Brushes 285 RamdhanieBao Tran NguyenNoch keine Bewertungen
- Guidelines For The Management of Brain InjuryDokument26 SeitenGuidelines For The Management of Brain InjuryfathaNoch keine Bewertungen
- Aesculap Saw GD307 - Service ManualDokument16 SeitenAesculap Saw GD307 - Service ManualFredi PançiNoch keine Bewertungen
- Cell Structure, Function Practice Test With AnswersDokument16 SeitenCell Structure, Function Practice Test With AnswersDJ ISAACSNoch keine Bewertungen
- Marketing Management 4th Edition Winer Test BankDokument35 SeitenMarketing Management 4th Edition Winer Test Bankapneaocheryzxs3ua100% (24)
- AR BuildingDokument819 SeitenAR BuildingShithin KrishnanNoch keine Bewertungen
- Accsap 10 VHDDokument94 SeitenAccsap 10 VHDMuhammad Javed Gaba100% (2)
- 40 RT-flex Control-System Rev01Dokument68 Seiten40 RT-flex Control-System Rev01Mayvon Botelho100% (2)
- Astm A194 2020Dokument12 SeitenAstm A194 2020rolando cuadro blancoNoch keine Bewertungen
- Zest O CorporationDokument21 SeitenZest O CorporationJhamane Chan53% (15)
- Tuesday, 16 November 2021 - Afternoon Discovering ElectronicsDokument20 SeitenTuesday, 16 November 2021 - Afternoon Discovering Electronicsnvmalt070Noch keine Bewertungen
- Opex and CapexDokument5 SeitenOpex and CapexATM Shafiq Ul AlamNoch keine Bewertungen
- Efficient Rice Based Cropping SystemDokument24 SeitenEfficient Rice Based Cropping Systemsenthilnathan100% (1)
- Banachek UnlimitedDokument34 SeitenBanachek UnlimitedserenaNoch keine Bewertungen
- Tesla Magazine Vol4Dokument48 SeitenTesla Magazine Vol4jonathan100% (1)
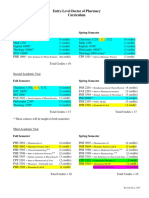
- Pharmd CurriculumDokument18 SeitenPharmd Curriculum5377773Noch keine Bewertungen
- Lecture5 PDE 2016Dokument22 SeitenLecture5 PDE 2016isele1977Noch keine Bewertungen
- Simple Roll-Type: A Loud SpeakerDokument1 SeiteSimple Roll-Type: A Loud SpeakerEudes SilvaNoch keine Bewertungen
- Pineapple in JohorDokument6 SeitenPineapple in JohorHaiqal AzizNoch keine Bewertungen
- Action Analysis For Animators by Chris WebsterDokument409 SeitenAction Analysis For Animators by Chris WebsterThomas Yandex100% (8)
- Differential Geometry of Curves and Surfaces 3. Regular SurfacesDokument16 SeitenDifferential Geometry of Curves and Surfaces 3. Regular SurfacesyrodroNoch keine Bewertungen
- Modern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaDokument2 SeitenModern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaKumar KumarNoch keine Bewertungen
- Vallarpadam Terminal ChallengesDokument3 SeitenVallarpadam Terminal Challengespriya rajeev100% (1)