Das könnte Ihnen auch gefallen
- Wound International Best Practice Guidelines Non ComplexDokument27 SeitenWound International Best Practice Guidelines Non ComplexEdu WilliamNoch keine Bewertungen
- Laser Guidance Notes 101212Dokument3 SeitenLaser Guidance Notes 101212Edu WilliamNoch keine Bewertungen
- PICU HandbookDokument113 SeitenPICU HandbookEdu WilliamNoch keine Bewertungen
- Dietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Dokument1 SeiteDietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Edu WilliamNoch keine Bewertungen
- Tanner MethodDokument8 SeitenTanner MethodEdu WilliamNoch keine Bewertungen
- CroupDokument13 SeitenCroupEdu William100% (1)
- Pedtext 5Dokument716 SeitenPedtext 5jay_eshwa100% (1)
- Japanese Encephalitis - 2011Dokument2 SeitenJapanese Encephalitis - 2011Edu WilliamNoch keine Bewertungen
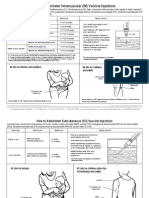
- How To Admister VaccineDokument2 SeitenHow To Admister VaccineEdu WilliamNoch keine Bewertungen
- Adenovirus Vaccine: What You Need To KnowDokument2 SeitenAdenovirus Vaccine: What You Need To KnowEdu WilliamNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Brain Cancer ThesisDokument7 SeitenBrain Cancer ThesisKristen Flores100% (2)
- Hepatitis C and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasDokument4 SeitenHepatitis C and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasBashir Mahmud Ellias100% (1)
- Kibi - DSTC - How To Keep The PT Alive I Juni 21Dokument32 SeitenKibi - DSTC - How To Keep The PT Alive I Juni 21tepat rshsNoch keine Bewertungen
- Anti EmesisDokument63 SeitenAnti EmesisOtilia SerescuNoch keine Bewertungen
- Dengue Hemorrhagic ShitDokument28 SeitenDengue Hemorrhagic ShitRebecca FabonNoch keine Bewertungen
- Pharma Biotech M A Transactions 2005-2012Dokument13 SeitenPharma Biotech M A Transactions 2005-2012Aniket ApteNoch keine Bewertungen
- Radiographic Standard Operating ProtocolsDokument220 SeitenRadiographic Standard Operating Protocolspurnima4uonlyNoch keine Bewertungen
- Buckinghamshire Pathways and Leaflets PDFDokument10 SeitenBuckinghamshire Pathways and Leaflets PDFAlexa SienesNoch keine Bewertungen
- Diagnostic Test in HematologyDokument18 SeitenDiagnostic Test in HematologyJOHN ARBIE TATTAO, RN100% (7)
- Terapi Cairain Dan ElektrolitDokument39 SeitenTerapi Cairain Dan ElektrolityulyaNoch keine Bewertungen
- Gynecological LaparosDokument32 SeitenGynecological LaparosYosef Dwi Cahyadi Salan100% (1)
- Bloodstream Infection MBDokument47 SeitenBloodstream Infection MBDarshan Koirala100% (1)
- Ÿ Sex-Biased AutoimmunityDokument31 SeitenŸ Sex-Biased AutoimmunityJessy NingNoch keine Bewertungen
- CH 1. Overview of The Immune SystemDokument23 SeitenCH 1. Overview of The Immune SystemIbrahim MNoch keine Bewertungen
- Piet AlDokument6 SeitenPiet AlKiara NurmathiasNoch keine Bewertungen
- Haramaya University College of Health and Medical Sciences School of Nursing and Midwifery MSC in Nursing (Major in Adult Health Nursing)Dokument54 SeitenHaramaya University College of Health and Medical Sciences School of Nursing and Midwifery MSC in Nursing (Major in Adult Health Nursing)Beyene Feleke100% (1)
- Factors Associated With Human Papillomavirus Related Stigma, Shame, and Intent of HPV TestDokument9 SeitenFactors Associated With Human Papillomavirus Related Stigma, Shame, and Intent of HPV TestChiboyKrenzNoch keine Bewertungen
- 227 235 SamamaDokument9 Seiten227 235 SamamayunitastyaningrumNoch keine Bewertungen
- NURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionDokument7 SeitenNURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media Submissionjoohnsmith070Noch keine Bewertungen
- The Effect of Uterine Closure Technique On Cesarean Scar Niche Development After Multiple Cesarean DeliveriesDokument8 SeitenThe Effect of Uterine Closure Technique On Cesarean Scar Niche Development After Multiple Cesarean DeliveriesWillans Eduardo Rosha HumerezNoch keine Bewertungen
- Tinjauan Pustaka: Respon Imunologi Pada Dermatitis Kontak IritanDokument7 SeitenTinjauan Pustaka: Respon Imunologi Pada Dermatitis Kontak IritanSatriadwykiyprasetya ThiodwkiyNoch keine Bewertungen
- Upload 29Dokument4 SeitenUpload 29Lenny SilalahiNoch keine Bewertungen
- Company ProfileDokument5 SeitenCompany ProfileHai HelloNoch keine Bewertungen
- Nursing Care PlansDokument16 SeitenNursing Care PlansSantos Kyla Patricia T.Noch keine Bewertungen
- Pathological Anatomy IntroductionDokument9 SeitenPathological Anatomy IntroductionRashid NawazNoch keine Bewertungen
- Imperforate AnusDokument52 SeitenImperforate Anushayssam rashwan100% (6)
- PhenylketonuriaDokument8 SeitenPhenylketonuriaAmberlee PetiNoch keine Bewertungen
- 1428567842PE-Perianal Fistula - GS - PE.01.0711Dokument2 Seiten1428567842PE-Perianal Fistula - GS - PE.01.0711Ronal GopeNoch keine Bewertungen
- Shaken Baby SyndromeDokument25 SeitenShaken Baby SyndromeArdanta Dat Topik TariganNoch keine Bewertungen
- Medication Information For Parents and Teachers: Atomoxetine-StratteraDokument8 SeitenMedication Information For Parents and Teachers: Atomoxetine-StratteraMonique WrightNoch keine Bewertungen