Das könnte Ihnen auch gefallen
- Naasadiiya PDFDokument4 SeitenNaasadiiya PDFabhishek kumar0% (1)
- 5112 Law 2 CriminalLaw-IIDokument264 Seiten5112 Law 2 CriminalLaw-IImayur860Noch keine Bewertungen
- Role of Timely Intervention in Preventing SuicideDokument72 SeitenRole of Timely Intervention in Preventing Suicideabhishek kumarNoch keine Bewertungen
- Geopolitics of Al Asad Regime in SyriaDokument94 SeitenGeopolitics of Al Asad Regime in Syriaabhishek kumarNoch keine Bewertungen
- Analysis BriberyDokument14 SeitenAnalysis BriberyPang Siew ChuNoch keine Bewertungen
- Near Hanging: PerspectivesDokument5 SeitenNear Hanging: Perspectivesabhishek kumarNoch keine Bewertungen
- Types of Business Associations Regulated by Mercantile LawDokument239 SeitenTypes of Business Associations Regulated by Mercantile Lawabhishek kumarNoch keine Bewertungen
- Importance of Capability and Intent in GeopoliticsDokument15 SeitenImportance of Capability and Intent in Geopoliticsabhishek kumarNoch keine Bewertungen
- Depression Learning PathDokument102 SeitenDepression Learning Pathabhishek kumarNoch keine Bewertungen
- Stopping For Death - Re-Framing Our Perspective On The End of LifeDokument53 SeitenStopping For Death - Re-Framing Our Perspective On The End of Lifeabhishek kumarNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Spirit Is Too Blunt An InstrumentDokument21 SeitenThe Spirit Is Too Blunt An InstrumentnellytusiimeNoch keine Bewertungen
- Asana Serie #1: 1. Urdhva HastasanaDokument43 SeitenAsana Serie #1: 1. Urdhva HastasanaAnonymous 4gamBfNoch keine Bewertungen
- Clinical Signs and TestsDokument7 SeitenClinical Signs and Testsmail2mohsinaliNoch keine Bewertungen
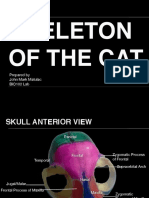
- Skeleton of The Cat: Prepared by John Mark Matulac BIO102 LabDokument27 SeitenSkeleton of The Cat: Prepared by John Mark Matulac BIO102 LabJoachimNoch keine Bewertungen
- Manual Therapy Paradigm Shift 2016Dokument11 SeitenManual Therapy Paradigm Shift 2016Tomáš KrajíčekNoch keine Bewertungen
- Bladder ExstrophyDokument37 SeitenBladder Exstrophymohamademil1983Noch keine Bewertungen
- 06 - Sullivan - A ReviewerDokument56 Seiten06 - Sullivan - A ReviewerCatrina Tan100% (2)
- Atlas of Osteopathic TechniquesDokument81 SeitenAtlas of Osteopathic TechniquesDanieleNoch keine Bewertungen
- Skeletal SystemDokument25 SeitenSkeletal SystemLeonard Soria GuanzonNoch keine Bewertungen
- Swim Bladder Malformation in Hatchery-Reared Striped Trumpeter Latris Lineata LatridaeDokument14 SeitenSwim Bladder Malformation in Hatchery-Reared Striped Trumpeter Latris Lineata LatridaenareNoch keine Bewertungen
- Recent Advances in ScoliosisDokument356 SeitenRecent Advances in ScoliosisLuigi PolitoNoch keine Bewertungen
- Peticao Inicial Restabelecimento B91 Concessao B92Dokument44 SeitenPeticao Inicial Restabelecimento B91 Concessao B92RENATANoch keine Bewertungen
- Medical Terminology PHARM TECHNICIANDokument215 SeitenMedical Terminology PHARM TECHNICIANCece RereNoch keine Bewertungen
- The Stabilizing System of The Spine Part 1..panjabiDokument7 SeitenThe Stabilizing System of The Spine Part 1..panjabilgminassianNoch keine Bewertungen
- Analgesia Epidural Current Views and ApproachesDokument168 SeitenAnalgesia Epidural Current Views and ApproachesManuel Ortega100% (2)
- KSM Orthopedi New1Dokument20 SeitenKSM Orthopedi New1rspku mayongNoch keine Bewertungen
- Efficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsDokument6 SeitenEfficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsthiagoNoch keine Bewertungen
- Fortinberry Chapter 1 - Clinical Application of Foundational SciencesDokument55 SeitenFortinberry Chapter 1 - Clinical Application of Foundational SciencesArianne Francesca GalaitesNoch keine Bewertungen
- Nerve Blocks BasicsDokument5 SeitenNerve Blocks BasicsAditi SharmaNoch keine Bewertungen
- Running Head: Using Metaphor To Teach Essay FormatDokument4 SeitenRunning Head: Using Metaphor To Teach Essay Formatapi-280086060Noch keine Bewertungen
- A Four-Legged Snake From The Early Cretaceous of GondwanaDokument6 SeitenA Four-Legged Snake From The Early Cretaceous of GondwanaYilbert Oswaldo Jimenez CanoNoch keine Bewertungen
- Gross Comparative Anatomy of Domestic AnimalsDokument51 SeitenGross Comparative Anatomy of Domestic AnimalsLila Loureen AlkuinoNoch keine Bewertungen
- E3 - OrthoDokument49 SeitenE3 - OrthoLuvleen KaurNoch keine Bewertungen
- ERA Nursing MSN Spinal Cord InjuryDokument7 SeitenERA Nursing MSN Spinal Cord InjuryAru Verma100% (1)
- Torticolis OdtDokument25 SeitenTorticolis OdtAndreea CimpoiNoch keine Bewertungen
- Vertebrates & Invertebrates: by Mariella Hany Grade 5 CDokument8 SeitenVertebrates & Invertebrates: by Mariella Hany Grade 5 CyoussefNoch keine Bewertungen
- Philippine Red Cross' Learn First Aid PDFDokument31 SeitenPhilippine Red Cross' Learn First Aid PDFCyrus Montalan73% (33)
- Solution Manual For Global Business Today, 11th Edition, Charles W. L. Hill, G. Tomas M. Hult, ISBN10: 1260088375, ISBN13: 9781260088373Dokument36 SeitenSolution Manual For Global Business Today, 11th Edition, Charles W. L. Hill, G. Tomas M. Hult, ISBN10: 1260088375, ISBN13: 9781260088373wartlessostmenew5xa2100% (12)
- Applied Anatomy of The Thorax and AbdomenDokument12 SeitenApplied Anatomy of The Thorax and AbdomenueumanaNoch keine Bewertungen
- Traction: Cervical & LumbarDokument21 SeitenTraction: Cervical & LumbarBoud ElhassanNoch keine Bewertungen