Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Plastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryDokument23 SeitenPlastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryTugce InceNoch keine Bewertungen
- Crio Combinada Com Outras TerapiasDokument6 SeitenCrio Combinada Com Outras TerapiasPolyana AlencarNoch keine Bewertungen
- Ailing and Failing Us Dental ImplantsDokument12 SeitenAiling and Failing Us Dental ImplantsCharlyBoeingNoch keine Bewertungen
- Zimmer Traction Handbook PDFDokument92 SeitenZimmer Traction Handbook PDFMarilyn100% (1)
- Geoffrey J. Gladstone, Frank A. Nesi, Evan H. Black - Oculoplastic Surgery Atlas - Cosmetic Facial Surgery-Springer (2018)Dokument77 SeitenGeoffrey J. Gladstone, Frank A. Nesi, Evan H. Black - Oculoplastic Surgery Atlas - Cosmetic Facial Surgery-Springer (2018)DANIEL GIRALDONoch keine Bewertungen
- Congenital Talipes Equino-VarusDokument48 SeitenCongenital Talipes Equino-VarusFera MulidarNoch keine Bewertungen
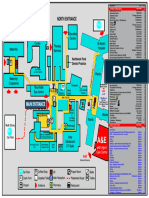
- Northwick Park Hospital Site MapDokument1 SeiteNorthwick Park Hospital Site MapHasaan KhanNoch keine Bewertungen
- Ultrasound Supraclavicular Plexus Block Enhances Arteriovenous Fistula Blood Flow in ESRDDokument14 SeitenUltrasound Supraclavicular Plexus Block Enhances Arteriovenous Fistula Blood Flow in ESRDaymankahlaNoch keine Bewertungen
- ALVO Operating TablesDokument44 SeitenALVO Operating Tablesvanxuong90Noch keine Bewertungen
- Awareness of Oral and Maxillofacial Surgery Among Healthcare Professionals in Kanpur - A Questionnaire Based StudyDokument7 SeitenAwareness of Oral and Maxillofacial Surgery Among Healthcare Professionals in Kanpur - A Questionnaire Based StudyInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- OrthoToolKit Anterior Cruciate Ligament Return To Sport After Injury (ACL-RSI) Calculator Score ReportDokument1 SeiteOrthoToolKit Anterior Cruciate Ligament Return To Sport After Injury (ACL-RSI) Calculator Score ReportfisiolhmarcelinoNoch keine Bewertungen
- Nursing Care of A Family With An Ill ChildDokument5 SeitenNursing Care of A Family With An Ill ChildAmna JalilNoch keine Bewertungen
- Rekap Umr 2019Dokument54 SeitenRekap Umr 2019Derri HafaNoch keine Bewertungen
- Gallstone Ileus PDFDokument4 SeitenGallstone Ileus PDFmonika100% (1)
- 18 COSM ProgramGuide Final PDFDokument76 Seiten18 COSM ProgramGuide Final PDFfluffy4202011Noch keine Bewertungen
- Witnesses and SponsorsDokument2 SeitenWitnesses and SponsorsdiazdizzamarieNoch keine Bewertungen
- Shunt Exposure As A Ventriculoperitoneal Shunt Complication A CaseDokument8 SeitenShunt Exposure As A Ventriculoperitoneal Shunt Complication A CasePutri Tamara DasantosNoch keine Bewertungen
- Rhomboid Flap - 2020 - Atlas of The Oral and Maxillofacial Surgery ClinicsDokument6 SeitenRhomboid Flap - 2020 - Atlas of The Oral and Maxillofacial Surgery Clinicslaljadeff12Noch keine Bewertungen
- Implant SystemsDokument103 SeitenImplant SystemsBharathi GudapatiNoch keine Bewertungen
- Health InfrastructureDokument23 SeitenHealth InfrastructureS raoNoch keine Bewertungen
- Pre Prosthetic Surgery PDFDokument107 SeitenPre Prosthetic Surgery PDFdrkavintNoch keine Bewertungen
- Flexible CO2 Laser Treatment For Subglottic Stenosis, 2017Dokument2 SeitenFlexible CO2 Laser Treatment For Subglottic Stenosis, 2017Araceli BarreraNoch keine Bewertungen
- Issa 2019Dokument6 SeitenIssa 2019İbrahim DemircioğluNoch keine Bewertungen
- OSCE Notes in Otology Surgery by DrtbaluDokument85 SeitenOSCE Notes in Otology Surgery by DrtbaluDrAli JafarNoch keine Bewertungen
- Supreme Health Brochure (Full Version)Dokument27 SeitenSupreme Health Brochure (Full Version)johnconnorNoch keine Bewertungen
- Fafaj2021 Tanaka Score ReliabilityDokument6 SeitenFafaj2021 Tanaka Score ReliabilityEham AroraNoch keine Bewertungen
- Wockhardt Hospitals: A Journey of Excellence in HealthcareDokument16 SeitenWockhardt Hospitals: A Journey of Excellence in HealthcarePuneet GuptaNoch keine Bewertungen
- Angiography Artis One Businesscase Brochure-02018163Dokument4 SeitenAngiography Artis One Businesscase Brochure-02018163TRUONG HOANG DUCNoch keine Bewertungen
- Uroso18 SynopsisDokument2 SeitenUroso18 SynopsiscaciorsNoch keine Bewertungen
- Career Resarch Part 2Dokument4 SeitenCareer Resarch Part 2api-478801132Noch keine Bewertungen