Das könnte Ihnen auch gefallen
- Adhesiveuseinoral Andmaxillofacial Surgery: Michael J. Buckley,, Eric J. BeckmanDokument5 SeitenAdhesiveuseinoral Andmaxillofacial Surgery: Michael J. Buckley,, Eric J. Beckmanhasan nazzalNoch keine Bewertungen
- DownloadDokument14 SeitenDownloadhasan nazzalNoch keine Bewertungen
- Computer-Assisted Craniomaxillofacial Surgery: Sean P. EdwardsDokument18 SeitenComputer-Assisted Craniomaxillofacial Surgery: Sean P. Edwardshasan nazzalNoch keine Bewertungen
- DownloadDokument12 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument22 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument12 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument9 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument13 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument10 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument15 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument16 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument18 SeitenDownloadhasan nazzalNoch keine Bewertungen
- DownloadDokument11 SeitenDownloadhasan nazzalNoch keine Bewertungen
- 1 s2.0 S1042369911000999 MainDokument11 Seiten1 s2.0 S1042369911000999 MaindrescobedocomfNoch keine Bewertungen
- Bonemorphogenetic Proteinsin Craniomaxillofacial Surgery: Sarah D. Davies,, Mark W. OchsDokument15 SeitenBonemorphogenetic Proteinsin Craniomaxillofacial Surgery: Sarah D. Davies,, Mark W. Ochshasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument3 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument10 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument10 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Outcomesresearch Andthechallenge Ofevidence-Based Surgery: Thomas B. DodsonDokument4 SeitenOutcomesresearch Andthechallenge Ofevidence-Based Surgery: Thomas B. Dodsonhasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument9 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument10 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument8 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument10 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument8 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- Clinics of North America 2011Dokument9 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- 1 s2.0 S1042369911001038 MainDokument8 Seiten1 s2.0 S1042369911001038 MaindrescobedocomfNoch keine Bewertungen
- Clinics of North America 2011Dokument6 SeitenClinics of North America 2011hasan nazzalNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Peds EORDokument29 SeitenPeds EORAndrew BowmanNoch keine Bewertungen
- Post Term PregnancyDokument22 SeitenPost Term PregnancyDarianne HernandezNoch keine Bewertungen
- Patient Management System PDFDokument3 SeitenPatient Management System PDFVamee AsuncionNoch keine Bewertungen
- E/M Audit Form: Chart #Dokument2 SeitenE/M Audit Form: Chart #Anthony El HageNoch keine Bewertungen
- Trametes Versicolor (Turkey Tail) For Breast and Other CancersDokument3 SeitenTrametes Versicolor (Turkey Tail) For Breast and Other Cancerssuperdave147Noch keine Bewertungen
- MDHA Write-Up For Prospective StudentsDokument1 SeiteMDHA Write-Up For Prospective StudentsprashantNoch keine Bewertungen
- Oral Habits and Its Relationship To Malocclusion A Review.20141212083000Dokument4 SeitenOral Habits and Its Relationship To Malocclusion A Review.20141212083000Stacia AnastashaNoch keine Bewertungen
- Medicine PDFDokument385 SeitenMedicine PDFMaheshNoch keine Bewertungen
- Identify The Strategies and Contextual Factors That Enable Optimal Engagement of Patients in The Design, Delivery, and Evaluation of Health ServicesDokument2 SeitenIdentify The Strategies and Contextual Factors That Enable Optimal Engagement of Patients in The Design, Delivery, and Evaluation of Health ServiceslouryNoch keine Bewertungen
- Admission and DischargeDokument3 SeitenAdmission and DischargePhilip Jay Braga100% (1)
- Introduction To Epidemiology & Public Health: Dr. Munibullah LecturerDokument22 SeitenIntroduction To Epidemiology & Public Health: Dr. Munibullah LecturerIbrar Faisal0% (1)
- Caregiver-Mediated Exercises With E-Health Support For Early Supported Discharge After Stroke (CARE4STROKE) : A Randomized Controlled TrialDokument15 SeitenCaregiver-Mediated Exercises With E-Health Support For Early Supported Discharge After Stroke (CARE4STROKE) : A Randomized Controlled TrialyenrilisnaNoch keine Bewertungen
- Pakistan Hand Hygiene For All Roadmap DocumentDokument30 SeitenPakistan Hand Hygiene For All Roadmap DocumentNiazullah KhanNoch keine Bewertungen
- History of LaparosDokument27 SeitenHistory of LaparosDr. Sanjay KolteNoch keine Bewertungen
- School StressDokument24 SeitenSchool StressShaheen Khan WarsiNoch keine Bewertungen
- ECPM 2021 European Congress of Perinatal MedicineDokument1 SeiteECPM 2021 European Congress of Perinatal MedicineAl DiNoch keine Bewertungen
- Initial Assessment: - Rambam Medical Center - DR Nordkin DmitriDokument60 SeitenInitial Assessment: - Rambam Medical Center - DR Nordkin Dmitridheviant12Noch keine Bewertungen
- Test Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full DownloadDokument24 SeitenTest Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full Downloadrobertabergmjnxqrasct100% (43)
- Medical Insurance Application Form: Icea General Insurance Company LimitedDokument2 SeitenMedical Insurance Application Form: Icea General Insurance Company LimitedKalyesubula Mahad AraaliNoch keine Bewertungen
- Empanelled Hospital List MedicareDokument608 SeitenEmpanelled Hospital List Medicaresid mahalo100% (1)
- Referat HIV AIDSDokument13 SeitenReferat HIV AIDSoctaviena zakariaNoch keine Bewertungen
- TB PDFDokument66 SeitenTB PDFKyaw Zin HtetNoch keine Bewertungen
- Dci Journal PointsDokument1 SeiteDci Journal PointsRajesh Rathod0% (1)
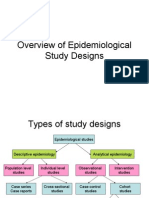
- Overview of Epidemiological Study DesignsDokument16 SeitenOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- Shimla Nursing College Annadale Bai BerbaiDokument17 SeitenShimla Nursing College Annadale Bai Berbaigill priyaNoch keine Bewertungen
- Activity Design COPC July6Dokument4 SeitenActivity Design COPC July6FAMED RESIDENTS CESMEDNoch keine Bewertungen
- Rights of Sewage Workers InterviewDokument8 SeitenRights of Sewage Workers Interviewapi-541981758Noch keine Bewertungen
- 3B - Clinical PharmacyDokument35 Seiten3B - Clinical PharmacyekramNoch keine Bewertungen
- Congenital Heart DiseaseDokument2 SeitenCongenital Heart DiseaseZAY EMNoch keine Bewertungen
- What Is Cancer PDFDokument5 SeitenWhat Is Cancer PDFBasitAfridiNoch keine Bewertungen