Das könnte Ihnen auch gefallen
- Setiawan 2015Dokument8 SeitenSetiawan 2015ShibaNoch keine Bewertungen
- Assignment 4Dokument5 SeitenAssignment 4NIKITA0% (1)
- Adoc - Pub Harborne J B Metode Fitokimia Penuntun Cara ModernDokument5 SeitenAdoc - Pub Harborne J B Metode Fitokimia Penuntun Cara ModernFirdaNoch keine Bewertungen
- Uji Stabilitas Formulasi Krim Tabir Surya Serbuk RUMPUT LAUT (Eucheuma Cottonii. Doty)Dokument4 SeitenUji Stabilitas Formulasi Krim Tabir Surya Serbuk RUMPUT LAUT (Eucheuma Cottonii. Doty)miftahulnazifahNoch keine Bewertungen
- Jurnal Maserasi Hal 5Dokument8 SeitenJurnal Maserasi Hal 5ElsiiNoch keine Bewertungen
- Identifikasi Hidrokuinon Pada Krim Pemutih Racikan Yang Beredar Di Pasar Tengah Bandar Lampung Secara Kromatografi Lapis Tipis (KLT)Dokument8 SeitenIdentifikasi Hidrokuinon Pada Krim Pemutih Racikan Yang Beredar Di Pasar Tengah Bandar Lampung Secara Kromatografi Lapis Tipis (KLT)Chandra YuniantoNoch keine Bewertungen
- Dipiro PneumoniaDokument8 SeitenDipiro Pneumoniameri dayaniNoch keine Bewertungen
- SPO High AlerTDokument19 SeitenSPO High AlerTHendraTriSaputroNoch keine Bewertungen
- Daftar Pustaka: Drug Substances and ProductsDokument2 SeitenDaftar Pustaka: Drug Substances and ProductsFaizah Min FadhlillahNoch keine Bewertungen
- 1099-1105 Ijpr1301179Dokument7 Seiten1099-1105 Ijpr1301179Indah Indryani UNoch keine Bewertungen
- FarmakokinetikaDokument142 SeitenFarmakokinetikaAstrid Bernadette Ulina PurbaNoch keine Bewertungen
- Analisis Deskriptif Efek Samping Penggunaan Obat Anti Tuberculosis Pada Pasien TBC Di Rsud Dr. Pirngadi MedanDokument7 SeitenAnalisis Deskriptif Efek Samping Penggunaan Obat Anti Tuberculosis Pada Pasien TBC Di Rsud Dr. Pirngadi MedanEva MelisaNoch keine Bewertungen
- Pharmacy Intravena Admixture Services (Pivas) : IV - Admixture Handling CytotoxicDokument32 SeitenPharmacy Intravena Admixture Services (Pivas) : IV - Admixture Handling CytotoxicintanNoch keine Bewertungen
- Indonesian FDA Regulations On Indonesian Traditional Nutraceuticals (Herbs) ContributorsDokument16 SeitenIndonesian FDA Regulations On Indonesian Traditional Nutraceuticals (Herbs) ContributorsDyva VanillaNoch keine Bewertungen
- Pert 3. Sediaan Radiofarmasi Dan RadiolabelingDokument19 SeitenPert 3. Sediaan Radiofarmasi Dan Radiolabelingwida safitrNoch keine Bewertungen
- Farmakologi FarmakodinamikDokument26 SeitenFarmakologi FarmakodinamikMuhammad Nikko AomadaniNoch keine Bewertungen
- Kuliah Colon DDS Reguler-Ganjil 2010 INDDokument125 SeitenKuliah Colon DDS Reguler-Ganjil 2010 INDYartiSulistiaNingratNoch keine Bewertungen
- Bromhexin Method of Analysis PDFDokument8 SeitenBromhexin Method of Analysis PDFJitendra YadavNoch keine Bewertungen
- Jurnal Rumus Kadar AbuDokument5 SeitenJurnal Rumus Kadar AbualyanuraNoch keine Bewertungen
- Biopharmaceutics Classification System-The Scientific Basis PDFDokument5 SeitenBiopharmaceutics Classification System-The Scientific Basis PDFtrianawidiacandra100% (1)
- Floor Stock AlamandaDokument2 SeitenFloor Stock AlamandayuliNoch keine Bewertungen
- Coek - Info - The Pharmaceutical Codex Principles and Practice oDokument1 SeiteCoek - Info - The Pharmaceutical Codex Principles and Practice oNomiNoch keine Bewertungen
- Ikatan Apoteker Indonesia (Iai) Cabang Kota BekasiDokument2 SeitenIkatan Apoteker Indonesia (Iai) Cabang Kota BekasichevyluvianaNoch keine Bewertungen
- JurnalDokument4 SeitenJurnallailaNoch keine Bewertungen
- Farmasi Industri: Stabilitas ObatDokument113 SeitenFarmasi Industri: Stabilitas ObatMelani JunaediNoch keine Bewertungen
- Review Jurnal Interaksi Obat Antihipertensi - Radhwa Fauztina (20190350050)Dokument13 SeitenReview Jurnal Interaksi Obat Antihipertensi - Radhwa Fauztina (20190350050)Radhwa FauztinaNoch keine Bewertungen
- Materi IAI Palangka Raya - Rev PDFDokument55 SeitenMateri IAI Palangka Raya - Rev PDFNopernas CahayaNoch keine Bewertungen
- 02-Pharmaceutical Care ProcessDokument42 Seiten02-Pharmaceutical Care ProcessBalsam Zahi Al-Hasan100% (1)
- Review On Prefilled Syringe As A Modern Technique For Packaging and Delivery of ParenteralDokument6 SeitenReview On Prefilled Syringe As A Modern Technique For Packaging and Delivery of ParenteralShivraj JadhavNoch keine Bewertungen
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDokument28 SeitenDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDwiPrasetyaningRahmawatiNoch keine Bewertungen
- A Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDokument11 SeitenA Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDinesh babuNoch keine Bewertungen
- Parameter FarmakokinetikDokument12 SeitenParameter FarmakokinetikNnay AnggraeniNoch keine Bewertungen
- Jurnal Review MegaDokument6 SeitenJurnal Review MegaLa OgaNoch keine Bewertungen
- PPDokument6 SeitenPPElvina iskandarNoch keine Bewertungen
- Dipiro Edisi 9 KolestrolDokument10 SeitenDipiro Edisi 9 KolestrolFriska tampuboLonNoch keine Bewertungen
- Artikel 1 PDFDokument9 SeitenArtikel 1 PDFsintiaNoch keine Bewertungen
- Prosedur Asli IodoformDokument3 SeitenProsedur Asli IodoformtartilaNoch keine Bewertungen
- Uji Aktivitas Antibakteri Kombinasi Minyak Atsiri Daun Gelam Putih (Melaleuca Leucadendra) Dan Rimpang Jahe (Zingiber Officinale) Terhadap Bakteri Staphylococcus Aureus Dan Escherichia Coli Secara inDokument74 SeitenUji Aktivitas Antibakteri Kombinasi Minyak Atsiri Daun Gelam Putih (Melaleuca Leucadendra) Dan Rimpang Jahe (Zingiber Officinale) Terhadap Bakteri Staphylococcus Aureus Dan Escherichia Coli Secara inberliana faradisaNoch keine Bewertungen
- Bio Evailabilitas Dan Bioekivalensi Aciclovir BABEDokument13 SeitenBio Evailabilitas Dan Bioekivalensi Aciclovir BABERian Nurdiana100% (1)
- Computational Methods For Prediction of Drug LikenessDokument10 SeitenComputational Methods For Prediction of Drug LikenesssciencystuffNoch keine Bewertungen
- Development and Validation of A Liquid Chromatography Method For The Analysis of Paromomycin Sulfate and Its Impurities 2155 9872.1000102Dokument4 SeitenDevelopment and Validation of A Liquid Chromatography Method For The Analysis of Paromomycin Sulfate and Its Impurities 2155 9872.1000102rbmoureNoch keine Bewertungen
- Expired DateDokument38 SeitenExpired DateAnggie Restyana100% (1)
- Monitoring Efek Samping ObatDokument8 SeitenMonitoring Efek Samping ObatWilujeng SulistyoriniNoch keine Bewertungen
- Daun LeilemDokument8 SeitenDaun Leilemniken retnoNoch keine Bewertungen
- Analisis Simetikon PDFDokument9 SeitenAnalisis Simetikon PDFArini Musfiroh50% (2)
- Pendekatan SOAP Farmasi KlinikDokument40 SeitenPendekatan SOAP Farmasi KlinikmadeNoch keine Bewertungen
- Kelompok 10 - Metode Optimasi Senyawa PenuntunDokument36 SeitenKelompok 10 - Metode Optimasi Senyawa Penuntunapr_aprililianti100% (1)
- KARAKTERISTIK TUGAS DAN TANGGUNG JAWAB APOTEKER MUSLIM - NewDokument30 SeitenKARAKTERISTIK TUGAS DAN TANGGUNG JAWAB APOTEKER MUSLIM - NewBantuinAku KakNoch keine Bewertungen
- Preformulasi AsetosalDokument2 SeitenPreformulasi AsetosalTazyinul Qoriah AlfauziahNoch keine Bewertungen
- Bab V Analisis Farmakoterapi - DRP 5.1 Lembar Pemakaian Obat Di IGDDokument16 SeitenBab V Analisis Farmakoterapi - DRP 5.1 Lembar Pemakaian Obat Di IGDCosmas ZebuaNoch keine Bewertungen
- CTM Direct CompressionDokument8 SeitenCTM Direct CompressionrizkamarNoch keine Bewertungen
- OPTIMASI ZAT WARNA BUNGA TELANG (Clitoria Ternatea) Sebagai Pewarna Alami Pada Sirup ParasetamolDokument9 SeitenOPTIMASI ZAT WARNA BUNGA TELANG (Clitoria Ternatea) Sebagai Pewarna Alami Pada Sirup ParasetamolReza Fadillah AchmadNoch keine Bewertungen
- Glimepiride TabletDokument48 SeitenGlimepiride Tabletrabd samNoch keine Bewertungen
- AHFS Drug InformationDokument10 SeitenAHFS Drug InformationMika FebryatiNoch keine Bewertungen
- 11 Farmakokinetika Klinik Antibiotika Aminoglikosida PDFDokument19 Seiten11 Farmakokinetika Klinik Antibiotika Aminoglikosida PDFIrfanSektionoNoch keine Bewertungen
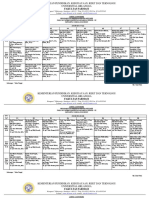
- Jadwal Ujian Sidang Periode 112 TGL 26-27 Juni 2021 (Rev)Dokument9 SeitenJadwal Ujian Sidang Periode 112 TGL 26-27 Juni 2021 (Rev)Yohan Nafisa NetNoch keine Bewertungen
- Coump & Disp (B - Latifah)Dokument101 SeitenCoump & Disp (B - Latifah)Muhammad Nurhadi Bin AbdulghaffarNoch keine Bewertungen
- Long-Acting Risperidone and Oral Antipsychotics in Unstable SchizophreniaDokument29 SeitenLong-Acting Risperidone and Oral Antipsychotics in Unstable SchizophreniahermanfirdausNoch keine Bewertungen
- Long-Acting Risperidone (1) .En - IdDokument10 SeitenLong-Acting Risperidone (1) .En - IdZidnil UlaNoch keine Bewertungen
- The Great Replacement The Violent Consequences of Mainstreamed Extremism by ISDDokument36 SeitenThe Great Replacement The Violent Consequences of Mainstreamed Extremism by ISDTom Lacovara-Stewart RTR TruthMediaNoch keine Bewertungen
- Summary of Evidence: Chicago Police Torture TrialDokument118 SeitenSummary of Evidence: Chicago Police Torture TrialAndres100% (1)
- NSTP (LTS) Activity 1 Ma. Nicole Pateño: 1. Give Your Own Perspective About The VMGO of BISU?Dokument3 SeitenNSTP (LTS) Activity 1 Ma. Nicole Pateño: 1. Give Your Own Perspective About The VMGO of BISU?MA. NICOLE PATENONoch keine Bewertungen
- State - CIF - Parent - Handbook - I - Understanding - Transfer - Elgibility - August - 2021-11 (Dragged) PDFDokument1 SeiteState - CIF - Parent - Handbook - I - Understanding - Transfer - Elgibility - August - 2021-11 (Dragged) PDFDaved BenefieldNoch keine Bewertungen
- Philosophy and National DevelopmentDokument8 SeitenPhilosophy and National DevelopmentIzo SeremNoch keine Bewertungen
- Tom Sawyer Vocabulary.1681608284879Dokument22 SeitenTom Sawyer Vocabulary.1681608284879Vhone NeyraNoch keine Bewertungen
- Social - Security - Net - TAMIL NADUDokument4 SeitenSocial - Security - Net - TAMIL NADUTamika LeeNoch keine Bewertungen
- SuccessionDokument47 SeitenSuccessionHyuga NejiNoch keine Bewertungen
- Manual Complex Engineering Problem: COMSATS University Islamabad Abbottabad CampusDokument35 SeitenManual Complex Engineering Problem: COMSATS University Islamabad Abbottabad CampusHajra SwatiNoch keine Bewertungen
- 56408e8ca7356 Allhoff 2003Dokument8 Seiten56408e8ca7356 Allhoff 2003yiğit tirkeşNoch keine Bewertungen
- A Poem For Cotton PickersDokument4 SeitenA Poem For Cotton Pickersapi-447987846Noch keine Bewertungen
- FLW Cronon Inconstant Unity Passion PDFDokument25 SeitenFLW Cronon Inconstant Unity Passion PDFAlexandraBarbieruNoch keine Bewertungen
- Internship Report NgoDokument14 SeitenInternship Report Ngosamarth chauhanNoch keine Bewertungen
- 6-Re - Petition For Radio and T.V. Coverage A.M. No. 10-11-5-SC, A.M. No. 10-11-6-SC and A.M. No. 10-11-7-SCDokument6 Seiten6-Re - Petition For Radio and T.V. Coverage A.M. No. 10-11-5-SC, A.M. No. 10-11-6-SC and A.M. No. 10-11-7-SCFelicity HuffmanNoch keine Bewertungen
- Melody Gardot Your Heart Is As Black As NightDokument8 SeitenMelody Gardot Your Heart Is As Black As NightmiruNoch keine Bewertungen
- Brij Pal Vs StateDokument7 SeitenBrij Pal Vs StateSatyendra ChauhanNoch keine Bewertungen
- Position PaperDokument9 SeitenPosition PaperJamellen De Leon BenguetNoch keine Bewertungen
- Jurnal Filsafat Hukum (Tri & Yusuf)Dokument5 SeitenJurnal Filsafat Hukum (Tri & Yusuf)vacefa2507Noch keine Bewertungen
- Assurance Principles, Professional Ethics and Good Governance SyllabusDokument15 SeitenAssurance Principles, Professional Ethics and Good Governance SyllabusGerlie0% (1)
- Session 5 - Marketing ManagementDokument6 SeitenSession 5 - Marketing ManagementJames MillsNoch keine Bewertungen
- Abs CBN vs. Ombudsman 2010Dokument11 SeitenAbs CBN vs. Ombudsman 2010Mara VinluanNoch keine Bewertungen
- Employment Contract: Prepared By: Atty. Daniel L. DiazDokument8 SeitenEmployment Contract: Prepared By: Atty. Daniel L. DiazKuya KimNoch keine Bewertungen
- Rakowski Complaint1 Amy MorrisDokument4 SeitenRakowski Complaint1 Amy Morrisapi-286623412Noch keine Bewertungen
- The Cincinnati Time Store As An Historical Precedent For Societal ChangeDokument11 SeitenThe Cincinnati Time Store As An Historical Precedent For Societal ChangeSteve Kemple100% (1)
- Deed of Assignment SM DavaoDokument2 SeitenDeed of Assignment SM DavaoFrancisqueteNoch keine Bewertungen
- Almirez Vs Infinite Loop TechnologyDokument2 SeitenAlmirez Vs Infinite Loop TechnologyJulian DubaNoch keine Bewertungen
- Business Communication 1Dokument13 SeitenBusiness Communication 1Kishan SrivastavaNoch keine Bewertungen
- Online Training of Trainers' (Tot) /walkthrough of Modules ScheduleDokument5 SeitenOnline Training of Trainers' (Tot) /walkthrough of Modules ScheduleJames Domini Lopez LabianoNoch keine Bewertungen
- b00105047 Posthuman Essay 2010Dokument14 Seitenb00105047 Posthuman Essay 2010Scott Brazil0% (1)
- NOSTALGIA - Grandma's Fridge Is Cool - Hemetsberger Kittiner e MullerDokument24 SeitenNOSTALGIA - Grandma's Fridge Is Cool - Hemetsberger Kittiner e MullerJúlia HernandezNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4.5 von 5 Sternen4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingVon EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingBewertung: 4 von 5 Sternen4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)