Das könnte Ihnen auch gefallen
- Life Histories of Genetic Disease: Patterns and Prevention in Postwar Medical GeneticsVon EverandLife Histories of Genetic Disease: Patterns and Prevention in Postwar Medical GeneticsNoch keine Bewertungen
- Section 1Dokument1 SeiteSection 1Nalie CortezNoch keine Bewertungen
- Metacognitive Reading Report STS ATANACIODokument2 SeitenMetacognitive Reading Report STS ATANACIOPatrick Atanacio0% (2)
- MRR 5 Tobias Ged104 BM1Dokument1 SeiteMRR 5 Tobias Ged104 BM1Haries Vi Traboc Micolob0% (1)
- Assessment Task-3Dokument8 SeitenAssessment Task-3JEROME NATIVIDAD50% (2)
- HickelDokument2 SeitenHickelYvonne Carol80% (10)
- Metacognitive Reading ReportDokument2 SeitenMetacognitive Reading Reportrjay manaloNoch keine Bewertungen
- HELIXDokument5 SeitenHELIXAljohn Asenci80% (5)
- Metacognitive Reading ReportDokument1 SeiteMetacognitive Reading ReportJoaquin Moulic0% (1)
- The Unleashing of A CrisisDokument13 SeitenThe Unleashing of A CrisisKyla Jadjurie100% (1)
- Causarin Act.3 Psychology 9.14-9.20Dokument2 SeitenCausarin Act.3 Psychology 9.14-9.20Denise CausarinNoch keine Bewertungen
- Metacognitive Reading ReportDokument2 SeitenMetacognitive Reading ReportEdrickMadlangbayan100% (3)
- Assignment Name: 1. Metacognitive Reading ReportDokument2 SeitenAssignment Name: 1. Metacognitive Reading Reportrjay manalo100% (1)
- Why The World Need WikileaksDokument2 SeitenWhy The World Need WikileaksMarwin Victoria67% (3)
- Lesson 4. When Technology and Humanity CrossDokument4 SeitenLesson 4. When Technology and Humanity CrossEde Shing100% (2)
- Exercise 1. Conceptualize A GMO: QuestionsDokument2 SeitenExercise 1. Conceptualize A GMO: Questionsrjay manalo100% (1)
- STS Assignment-5-The-fate-of-the-Philippine-Science-and-Technology-Innovation.Dokument2 SeitenSTS Assignment-5-The-fate-of-the-Philippine-Science-and-Technology-Innovation.Asuna Yuuki50% (2)
- Assignment 4. Metacognitive Reading ReportDokument2 SeitenAssignment 4. Metacognitive Reading ReportTherese Janine HetutuaNoch keine Bewertungen
- Ano ULOdDokument4 SeitenAno ULOdyes yesnoNoch keine Bewertungen
- Bernales M3S5 Assignment13Dokument2 SeitenBernales M3S5 Assignment13Therese Janine Hetutua100% (1)
- Metacognitive Reading Report 2Dokument2 SeitenMetacognitive Reading Report 2Melvin Dayao100% (1)
- Task Compilation (TC) 1Dokument8 SeitenTask Compilation (TC) 1Karen Britanico100% (1)
- STS ISSUES IN SCIENCE AND TECHNOLOGY - STS Assignment 2Dokument2 SeitenSTS ISSUES IN SCIENCE AND TECHNOLOGY - STS Assignment 2Asuna YuukiNoch keine Bewertungen
- Lesson 1Dokument2 SeitenLesson 1rjay manalo50% (8)
- MRR3Dokument2 SeitenMRR3Patrick Antonio Orge Ching60% (5)
- STS - Assignment 7-Caoli OliviaDokument2 SeitenSTS - Assignment 7-Caoli OliviaAsuna Yuuki50% (6)
- MedicinemanDokument1 SeiteMedicinemanYna WenceslaoNoch keine Bewertungen
- Exercise 2. Documentary Video Production: (I'll Send The Video in Separate File)Dokument2 SeitenExercise 2. Documentary Video Production: (I'll Send The Video in Separate File)rjay manalo100% (5)
- Metacognitive Reading Report Template-STS-1Dokument1 SeiteMetacognitive Reading Report Template-STS-1joy lopez100% (1)
- Advantages and Disadvantages Manipulation of Atoms and MoleculesDokument1 SeiteAdvantages and Disadvantages Manipulation of Atoms and MoleculesMariecris BatasNoch keine Bewertungen
- STS ReportDokument26 SeitenSTS ReportJae Ryan PitacioNoch keine Bewertungen
- Let's Check Activity 1Dokument3 SeitenLet's Check Activity 1Chang DrilonNoch keine Bewertungen
- Task Compilation (TC) 2Dokument3 SeitenTask Compilation (TC) 2Karen BritanicoNoch keine Bewertungen
- Bubble Kid - Success Puts Gene Therapy Back On TrackDokument2 SeitenBubble Kid - Success Puts Gene Therapy Back On TrackAngelica BaldresNoch keine Bewertungen
- That Sugar Film Discussion GuideDokument5 SeitenThat Sugar Film Discussion GuideGabriela arinque100% (2)
- Chapter 3 Unit 4 STS Courseware 1Dokument30 SeitenChapter 3 Unit 4 STS Courseware 1Jimbo ManalastasNoch keine Bewertungen
- MRR STSDokument2 SeitenMRR STSSabria Enriquez100% (8)
- Lesson 9Dokument2 SeitenLesson 9rjay manaloNoch keine Bewertungen
- Exercise 1 - Conceptualize A GMODokument2 SeitenExercise 1 - Conceptualize A GMOKO JI AN DO (Fries)Noch keine Bewertungen
- Ransom WareDokument2 SeitenRansom WareAjing Goblok100% (2)
- Lea Jane G. Cadano BSA 1-A: ElaborateDokument2 SeitenLea Jane G. Cadano BSA 1-A: ElaborateLea Jane CadanoNoch keine Bewertungen
- 1.assignment - Documentary Film AnalysisDokument1 Seite1.assignment - Documentary Film Analysisantonio aban100% (3)
- THE Textalyzer: Ines, Jeremieah Torres, Alicia Yap, Jairra Zamora, JosephDokument6 SeitenTHE Textalyzer: Ines, Jeremieah Torres, Alicia Yap, Jairra Zamora, Josephbianca reyesNoch keine Bewertungen
- Ccording To Studies of Scientists and From The Short Documentary Film, "Panahon Na! Ang Hamon Sa Pinoy at Climate Change,"Dokument2 SeitenCcording To Studies of Scientists and From The Short Documentary Film, "Panahon Na! Ang Hamon Sa Pinoy at Climate Change,"Yna WenceslaoNoch keine Bewertungen
- Exercise 3. Essay: "The Impact of Information Revolution To Local and Global Peace and Security"Dokument2 SeitenExercise 3. Essay: "The Impact of Information Revolution To Local and Global Peace and Security"rjay manalo100% (4)
- Final Individual Assignment - Cultural Beliefs On Disease Causation in The PhilippinesDokument4 SeitenFinal Individual Assignment - Cultural Beliefs On Disease Causation in The PhilippinesRiany IgnacioNoch keine Bewertungen
- Bubble KidDokument1 SeiteBubble Kidchristina marie salakNoch keine Bewertungen
- EnviDokument21 SeitenEnviRalf NapolesNoch keine Bewertungen
- Sts (Tapos Na) Benito LumenDokument1 SeiteSts (Tapos Na) Benito LumenCzad Fered Gilhang0% (1)
- Science, Technology and Society: (MIDTERM Lesson 1-5)Dokument4 SeitenScience, Technology and Society: (MIDTERM Lesson 1-5)Kyla Gatus89% (9)
- M1 Section 1. Assignment 1 Metacognitive Reading ReportDokument2 SeitenM1 Section 1. Assignment 1 Metacognitive Reading ReportLandThere100% (1)
- Vinluan, Jericho P. Midterm Activity 1Dokument2 SeitenVinluan, Jericho P. Midterm Activity 1jek vinNoch keine Bewertungen
- Metacognitive Reading Report # - : (What Concepts Did You Find Difficult To Understand?)Dokument2 SeitenMetacognitive Reading Report # - : (What Concepts Did You Find Difficult To Understand?)Jennie KimNoch keine Bewertungen
- Instructions: On The Box Provided, Draw A Possible GMO. in Conceptualizing A GMO, Think ofDokument1 SeiteInstructions: On The Box Provided, Draw A Possible GMO. in Conceptualizing A GMO, Think ofRM VlogsNoch keine Bewertungen
- In A Nutshell (Activity 2) GE5Dokument1 SeiteIn A Nutshell (Activity 2) GE5Rutchelle Desiree SenadonNoch keine Bewertungen
- RE 113 Integration: Submitted To: Sir Jose Suizo Submitted By: Jocelly TupasDokument8 SeitenRE 113 Integration: Submitted To: Sir Jose Suizo Submitted By: Jocelly TupasJacie TupasNoch keine Bewertungen
- Cherie Mae B Fuentes SECTION 2 p.81: Human Flourishing in Progress and De-DevelopmentDokument2 SeitenCherie Mae B Fuentes SECTION 2 p.81: Human Flourishing in Progress and De-DevelopmentyoyoyoNoch keine Bewertungen
- Exercise 1Dokument2 SeitenExercise 1Chris CiervoNoch keine Bewertungen
- Elsi rDNA TechnologyDokument4 SeitenElsi rDNA TechnologyLeena DraviamNoch keine Bewertungen
- Assignment 4 - "Derivatives"Dokument2 SeitenAssignment 4 - "Derivatives"Yaman PaliwalNoch keine Bewertungen
- Chapter 5. Everything Needs To Be SecuredDokument25 SeitenChapter 5. Everything Needs To Be SecuredCHUA CHONG SHENNoch keine Bewertungen
- Growing Leaders Certificate Cat 1Dokument4 SeitenGrowing Leaders Certificate Cat 1Ann OkothNoch keine Bewertungen
- Philpot v. Rural Media Group - Willie Nelson Photo PDFDokument9 SeitenPhilpot v. Rural Media Group - Willie Nelson Photo PDFMark JaffeNoch keine Bewertungen
- Energy Management Solutions - CatalogueDokument56 SeitenEnergy Management Solutions - CatalogueShilpa GharatNoch keine Bewertungen
- TSPSC QuestionsDokument172 SeitenTSPSC Questions68tq4dhm8pNoch keine Bewertungen
- Art 74 Marriage Settlement Ante Nuptial AgreementDokument5 SeitenArt 74 Marriage Settlement Ante Nuptial AgreementCelest AtasNoch keine Bewertungen
- (Routledge Research in Higher Education) Jenny L. Small - Critical Religious Pluralism in Higher Education - A Social Justice Framework To Support Religious Diversity-Routledge (2020)Dokument105 Seiten(Routledge Research in Higher Education) Jenny L. Small - Critical Religious Pluralism in Higher Education - A Social Justice Framework To Support Religious Diversity-Routledge (2020)yakadimaya43Noch keine Bewertungen
- Labrador vs. Court of Appeals, April 5, 1990Dokument2 SeitenLabrador vs. Court of Appeals, April 5, 1990Karen Sheila B. Mangusan - Degay100% (1)
- G.R. No. 152392 May 26, 2005 EXPERTRAVEL & TOURS, INC., Petitioner, Court of Appeals and Korean Airlines, RespondentDokument34 SeitenG.R. No. 152392 May 26, 2005 EXPERTRAVEL & TOURS, INC., Petitioner, Court of Appeals and Korean Airlines, RespondentNaiza Mae R. BinayaoNoch keine Bewertungen
- Principle of Least Privilege (POLP) : What, Why & Best PracticesDokument4 SeitenPrinciple of Least Privilege (POLP) : What, Why & Best PracticesManikanta Sai KumarNoch keine Bewertungen
- SAP For SCM OTIF Improvement ProjectDokument5 SeitenSAP For SCM OTIF Improvement ProjectMANOJNoch keine Bewertungen
- E-Goverment Opportunities and ChallengesDokument24 SeitenE-Goverment Opportunities and ChallengesMikaye WrightNoch keine Bewertungen
- ABC Elearning WorkbookDokument11 SeitenABC Elearning Workbooksacascasc0% (1)
- Theory and Practice in Language StudiesDokument170 SeitenTheory and Practice in Language StudiesHossam Abd-ElghafarNoch keine Bewertungen
- Community Participation in Development ProjectsDokument52 SeitenCommunity Participation in Development ProjectsRuby GarciaNoch keine Bewertungen
- Legal in MedievalDokument196 SeitenLegal in MedievalHabib ManzerNoch keine Bewertungen
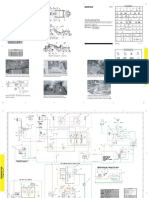
- Esquema Hidráulico Trailla 631GDokument2 SeitenEsquema Hidráulico Trailla 631GJose Carlos Annicchiarico BritoNoch keine Bewertungen
- VC Arun Prasad: Manager - Marketing (International Business)Dokument4 SeitenVC Arun Prasad: Manager - Marketing (International Business)rameshshNoch keine Bewertungen
- Information System AnalysisDokument12 SeitenInformation System AnalysisTosin WilliamsNoch keine Bewertungen
- What I Want To Accomplish While in JapanDokument1 SeiteWhat I Want To Accomplish While in JapanLariah LegadaNoch keine Bewertungen
- Sample of Consignment Format PDFDokument1 SeiteSample of Consignment Format PDFBeatrice JayNoch keine Bewertungen
- Economics SQPDokument7 SeitenEconomics SQPKanchana RamaiyaNoch keine Bewertungen
- Liquipoint T FTW31, FTW32: Operating InstructionsDokument32 SeitenLiquipoint T FTW31, FTW32: Operating InstructionssapesajeNoch keine Bewertungen
- SSM English CatalogueDokument196 SeitenSSM English CatalogueSELCUK ONUKNoch keine Bewertungen
- Ib History HL Revision Work BookDokument69 SeitenIb History HL Revision Work Bookapi-239922881Noch keine Bewertungen
- Tax 1 - Dean's Circle 2019 22Dokument1 SeiteTax 1 - Dean's Circle 2019 22Romeo G. Labador Jr.Noch keine Bewertungen
- 8milam ItcDokument1 Seite8milam Itcatishi88Noch keine Bewertungen
- Managerial Accounting 8th Edition: Chapter 11 SolutionsDokument25 SeitenManagerial Accounting 8th Edition: Chapter 11 SolutionsMarielle Tamayo100% (1)
- As ISO IEC 11179.5-2005 Information Technology - Metadata Registries (MDR) Naming and Identification PrinciplDokument8 SeitenAs ISO IEC 11179.5-2005 Information Technology - Metadata Registries (MDR) Naming and Identification PrinciplSAI Global - APACNoch keine Bewertungen
- Easyway Express: Stop Smoking and Quit E-CigarettesVon EverandEasyway Express: Stop Smoking and Quit E-CigarettesBewertung: 5 von 5 Sternen5/5 (15)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousVon EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousBewertung: 5 von 5 Sternen5/5 (22)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionVon EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductVon EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductBewertung: 5 von 5 Sternen5/5 (31)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryVon EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryBewertung: 5 von 5 Sternen5/5 (47)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingVon EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingBewertung: 5 von 5 Sternen5/5 (11)
- We Are the Luckiest: The Surprising Magic of a Sober LifeVon EverandWe Are the Luckiest: The Surprising Magic of a Sober LifeBewertung: 5 von 5 Sternen5/5 (183)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildVon EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildBewertung: 3.5 von 5 Sternen3.5/5 (9)
- Intoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingVon EverandIntoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingBewertung: 5 von 5 Sternen5/5 (1)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryVon EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNoch keine Bewertungen
- Stop Drinking Now: The original Easyway methodVon EverandStop Drinking Now: The original Easyway methodBewertung: 5 von 5 Sternen5/5 (29)
- Guts: The Endless Follies and Tiny Triumphs of a Giant DisasterVon EverandGuts: The Endless Follies and Tiny Triumphs of a Giant DisasterBewertung: 4 von 5 Sternen4/5 (99)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsVon EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNoch keine Bewertungen
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerVon EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerBewertung: 5 von 5 Sternen5/5 (8)
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsVon EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsBewertung: 4.5 von 5 Sternen4.5/5 (6)
- Living Sober: Practical methods alcoholics have used for living without drinkingVon EverandLiving Sober: Practical methods alcoholics have used for living without drinkingBewertung: 4 von 5 Sternen4/5 (50)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholVon EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholBewertung: 4 von 5 Sternen4/5 (6)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Von EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Bewertung: 4 von 5 Sternen4/5 (7)
- Stop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenVon EverandStop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenBewertung: 5 von 5 Sternen5/5 (62)
- 12 Step Spirituality: Every Person’s Guide to Taking the Twelve StepsVon Everand12 Step Spirituality: Every Person’s Guide to Taking the Twelve StepsBewertung: 5 von 5 Sternen5/5 (17)
- Addiction and Grace: Love and Spirituality in the Healing of AddictionsVon EverandAddiction and Grace: Love and Spirituality in the Healing of AddictionsBewertung: 4.5 von 5 Sternen4.5/5 (11)
- The Easy Way to Stop Gambling: Take Control of Your LifeVon EverandThe Easy Way to Stop Gambling: Take Control of Your LifeBewertung: 4 von 5 Sternen4/5 (197)