Das könnte Ihnen auch gefallen
- Qihan NVR User Manual-V1.2Dokument107 SeitenQihan NVR User Manual-V1.2sersehNoch keine Bewertungen
- Example of Well Written Interpretation RequestsDokument3 SeitenExample of Well Written Interpretation RequestssersehNoch keine Bewertungen
- BPV Certification Form New ApplicationDokument9 SeitenBPV Certification Form New ApplicationHoque AnamulNoch keine Bewertungen
- Propension of Materials To Retain Ash Forming Elements - SinteringDokument68 SeitenPropension of Materials To Retain Ash Forming Elements - SinteringsersehNoch keine Bewertungen
- How To Choose Your Personal SuccessDokument15 SeitenHow To Choose Your Personal SuccessBlackmorthNoch keine Bewertungen
- Jar of Beans - ChangelogDokument5 SeitenJar of Beans - ChangelogGomzalez Bin GembozNoch keine Bewertungen
- As 12042 - Es Refugios Peatonales (1) - Rev2Dokument1 SeiteAs 12042 - Es Refugios Peatonales (1) - Rev2sersehNoch keine Bewertungen
- Sir10sa ManualDokument48 SeitenSir10sa ManualsersehNoch keine Bewertungen
- Effect of Pre-Steaming and Impregnation On The Eucalyptus Pulp Cooking Yield 23082010Dokument27 SeitenEffect of Pre-Steaming and Impregnation On The Eucalyptus Pulp Cooking Yield 23082010sersehNoch keine Bewertungen
- ASTM - D3370-95a Standards Practices For Sampling Water From Closed ConduitsDokument11 SeitenASTM - D3370-95a Standards Practices For Sampling Water From Closed ConduitssersehNoch keine Bewertungen
- Comprehensive Look at Conductivity Measurement in Steam and Power GenerationDokument11 SeitenComprehensive Look at Conductivity Measurement in Steam and Power GenerationsersehNoch keine Bewertungen
- Report titleDokument25 SeitenReport titlesersehNoch keine Bewertungen
- Chip Preparation and Chip Properties - No RecomendationsDokument13 SeitenChip Preparation and Chip Properties - No RecomendationssersehNoch keine Bewertungen
- Medicinas Alternativas Glomerulonefritis PDFDokument13 SeitenMedicinas Alternativas Glomerulonefritis PDFsersehNoch keine Bewertungen
- ASTM - D3370-95a Standards Practices For Sampling Water From Closed ConduitsDokument11 SeitenASTM - D3370-95a Standards Practices For Sampling Water From Closed ConduitssersehNoch keine Bewertungen
- 0 - Initialization Cover PageDokument1 Seite0 - Initialization Cover PagesersehNoch keine Bewertungen
- Sealing Water Pump Testing and Operation Start - AC Rev. DGT 13.06.07Dokument5 SeitenSealing Water Pump Testing and Operation Start - AC Rev. DGT 13.06.07sersehNoch keine Bewertungen
- TERO3Dokument38 SeitenTERO3sersehNoch keine Bewertungen
- Intro HakonenDokument245 SeitenIntro HakonensersehNoch keine Bewertungen
- Ejemplo 1Dokument5 SeitenEjemplo 1sersehNoch keine Bewertungen
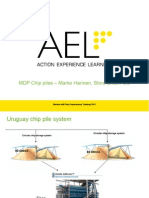
- Chip Piles Part M HarinenDokument10 SeitenChip Piles Part M HarinensersehNoch keine Bewertungen
- Chip Piles Part M HarinenDokument10 SeitenChip Piles Part M HarinensersehNoch keine Bewertungen
- NACE - Jubail GEWPT1Dokument37 SeitenNACE - Jubail GEWPT1riccardocozzaNoch keine Bewertungen
- SP Engineering Manual LOW EngDokument47 SeitenSP Engineering Manual LOW EngGROIIM100% (2)
- Exercise 1: Montes Del Plata Supervisory Training 2011Dokument7 SeitenExercise 1: Montes Del Plata Supervisory Training 2011sersehNoch keine Bewertungen
- Vectra XL CPD SheetDokument1 SeiteVectra XL CPD SheetLuis Angel Cuevas OrtegaNoch keine Bewertungen
- Montes Del Plata Supervisory Training: Personal Target SettingDokument14 SeitenMontes Del Plata Supervisory Training: Personal Target SettingsersehNoch keine Bewertungen
- Montes Del Plata Supervisory Training: PTS2Dokument16 SeitenMontes Del Plata Supervisory Training: PTS2sersehNoch keine Bewertungen
- Fic 0001Dokument1 SeiteFic 0001sersehNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- PositionsDokument4 SeitenPositionsMixsz LlhAdyNoch keine Bewertungen
- Round Warre HivesDokument16 SeitenRound Warre HivesBender Rodríguez100% (1)
- How Time Management Impacts Working Students' Academic AchievementDokument13 SeitenHow Time Management Impacts Working Students' Academic AchievementJames RayNoch keine Bewertungen
- TST-13 Aircraft Manual With 503 Engine LSA Rev.1Dokument52 SeitenTST-13 Aircraft Manual With 503 Engine LSA Rev.1smeassick100% (1)
- Butonal NS 175 TDSDokument2 SeitenButonal NS 175 TDSPT. PITAGORAS KONSULTANNoch keine Bewertungen
- Higuey, Dom Rep Mdpc/Puj: .Eff.23.MayDokument5 SeitenHiguey, Dom Rep Mdpc/Puj: .Eff.23.MayVanessa Yumayusa0% (1)
- The Dukan Diet by Dr. Pierre Dukan - ExcerptDokument8 SeitenThe Dukan Diet by Dr. Pierre Dukan - ExcerptCrown Publishing Group15% (20)
- Masagana High School: Module 4: Planning For Continuing Professional Development and Lac PlanningDokument6 SeitenMasagana High School: Module 4: Planning For Continuing Professional Development and Lac PlanningjhonaNoch keine Bewertungen
- Gpat 2014 SolvedDokument12 SeitenGpat 2014 Solvedjhansi100% (1)
- Battery: Ultrasonic Welding TechnologyDokument12 SeitenBattery: Ultrasonic Welding TechnologyNam Cao HuỳnhNoch keine Bewertungen
- Cape Vincent Area Events January 2019Dokument5 SeitenCape Vincent Area Events January 2019NewzjunkyNoch keine Bewertungen
- Pre Mocks Y11 2023Dokument14 SeitenPre Mocks Y11 2023Ahsan AhmedNoch keine Bewertungen
- CAPE Biology 2006 U2 P1 PDFDokument28 SeitenCAPE Biology 2006 U2 P1 PDFvedant seerattanNoch keine Bewertungen
- Do We Still Need Formocresol in Pediatric DentistryDokument3 SeitenDo We Still Need Formocresol in Pediatric DentistryAlexanderDetorakisNoch keine Bewertungen
- ACCT 4410 Taxation Salaries tax (Part II) Key areasDokument40 SeitenACCT 4410 Taxation Salaries tax (Part II) Key areasElaine LingxNoch keine Bewertungen
- TN EpasssDokument2 SeitenTN EpasssStephenrajNoch keine Bewertungen
- Different Types of Volcanic HazardsDokument5 SeitenDifferent Types of Volcanic HazardsJohn Carlo BañasNoch keine Bewertungen
- Exp. 5 Test For Fats and ProteinsDokument6 SeitenExp. 5 Test For Fats and ProteinsEMELIE GRACE E CACHERONoch keine Bewertungen
- 1 s2.0 S2667345222000104 MainDokument19 Seiten1 s2.0 S2667345222000104 MainJosiah MwashitaNoch keine Bewertungen
- HemophiliaDokument62 SeitenHemophiliamuhirwa Samuel100% (1)
- JSS20-48 Single Time Control Digital Display Time Relay: Page 1 / 2Dokument2 SeitenJSS20-48 Single Time Control Digital Display Time Relay: Page 1 / 2FranciscoNoch keine Bewertungen
- ITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsDokument1 SeiteITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsShashank JainNoch keine Bewertungen
- Evonik Copi BrochureDokument5 SeitenEvonik Copi BrochureRovshan HasanzadeNoch keine Bewertungen
- Process Industry Practices Structural: PIP STC01015 Structural Design CriteriaDokument16 SeitenProcess Industry Practices Structural: PIP STC01015 Structural Design CriteriaHarjasa AdhiNoch keine Bewertungen
- ECD KEBVF5 Installation ManualDokument32 SeitenECD KEBVF5 Installation Manualashish gautamNoch keine Bewertungen
- Piling Procedure - IoclDokument8 SeitenPiling Procedure - IocltpgggkNoch keine Bewertungen
- PKL Geri RevDokument3 SeitenPKL Geri RevKurniati NiaNoch keine Bewertungen
- Pronunciation Pairs Unit 2-6 Answer KeyDokument5 SeitenPronunciation Pairs Unit 2-6 Answer KeyChloe Liu50% (2)
- Multiple Choice RadioactivityDokument4 SeitenMultiple Choice RadioactivityGodhrawala AliasgerNoch keine Bewertungen
- Stick LoggerDokument2 SeitenStick LoggerjoseNoch keine Bewertungen