Das könnte Ihnen auch gefallen
- ENBS Basic Info Brochure 012015Dokument1 SeiteENBS Basic Info Brochure 012015Jessieka Marie Lina LayaNoch keine Bewertungen
- Change Name RequestDokument1 SeiteChange Name RequestJessieka Marie Lina LayaNoch keine Bewertungen
- Buntis Day: Cho Cabanatuan City/ Rhu I Mayapyap SurDokument4 SeitenBuntis Day: Cho Cabanatuan City/ Rhu I Mayapyap SurJessieka Marie Lina LayaNoch keine Bewertungen
- DOH AO 2010 0014 Administration of Life-Saving Drugs and Medicine by Midwives-1Dokument6 SeitenDOH AO 2010 0014 Administration of Life-Saving Drugs and Medicine by Midwives-1maxicap7367% (6)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Lesson Plan: Farhana Ahasan Assistant Professor Dept. of English Stamford University BangladeshDokument37 SeitenLesson Plan: Farhana Ahasan Assistant Professor Dept. of English Stamford University BangladeshMd SarroarNoch keine Bewertungen
- Literature Review With NvivoDokument6 SeitenLiterature Review With Nvivoafmzmqwdglhzex100% (1)
- Virtue Ethics FinalDokument19 SeitenVirtue Ethics FinalAlna JaeNoch keine Bewertungen
- Chapter 1 RevisedDokument7 SeitenChapter 1 RevisedChristian PalmosNoch keine Bewertungen
- Laser TB CoverDokument2 SeitenLaser TB CoverNarine Hovhannisyan0% (1)
- ENG03Dokument2 SeitenENG03Fatima SantosNoch keine Bewertungen
- Nur Hepsanti Hasanah: EducationDokument2 SeitenNur Hepsanti Hasanah: EducationMuhammad Mizan AbhiyasaNoch keine Bewertungen
- High School Report CardDokument2 SeitenHigh School Report Cardapi-517873514Noch keine Bewertungen
- Operator's Manual V3.0: FGRDEI01.fm Page - 1 Tuesday, November 12, 2002 2:04 PMDokument14 SeitenOperator's Manual V3.0: FGRDEI01.fm Page - 1 Tuesday, November 12, 2002 2:04 PMDumitru CristianNoch keine Bewertungen
- TOEFL Writing PDF PDFDokument40 SeitenTOEFL Writing PDF PDFFaz100% (1)
- Test 1011Dokument5 SeitenTest 1011Sieun LeeNoch keine Bewertungen
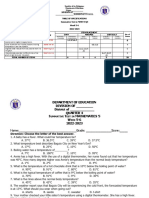
- ST3 - Math 5 - Q4Dokument3 SeitenST3 - Math 5 - Q4Maria Angeline Delos SantosNoch keine Bewertungen
- Prasad S Ambalkar ResumeDokument2 SeitenPrasad S Ambalkar Resumep1440666Noch keine Bewertungen
- Engineering Industrial Training Student Guide SpreadDokument11 SeitenEngineering Industrial Training Student Guide SpreadAkaash TangNoch keine Bewertungen
- Bystander Effect Corpuz&Reyes BSPsyIIIDokument16 SeitenBystander Effect Corpuz&Reyes BSPsyIIIJanine Mae Villostas CorpuzNoch keine Bewertungen
- Foundation of Curriculum DevelopmentDokument37 SeitenFoundation of Curriculum DevelopmentEddiely OlvidoNoch keine Bewertungen
- Mark Scheme (Results) November 2020: Pearson Edexcel International GCSE Mathematics A (4MA1) Paper 2HDokument21 SeitenMark Scheme (Results) November 2020: Pearson Edexcel International GCSE Mathematics A (4MA1) Paper 2HSteve TeeNoch keine Bewertungen
- TA in PsychotherapyDokument37 SeitenTA in PsychotherapyJesús RiveraNoch keine Bewertungen
- Mid-Term Assignment - Sun SimaDokument2 SeitenMid-Term Assignment - Sun SimaSima SunNoch keine Bewertungen
- MBA in Healthcare Management - Masters in Hospital AdministrationDokument2 SeitenMBA in Healthcare Management - Masters in Hospital AdministrationSandeep SonawneNoch keine Bewertungen
- My Favorite Meal EssayDokument7 SeitenMy Favorite Meal Essayb71g37ac100% (2)
- Release Management Processes (Article) PDFDokument14 SeitenRelease Management Processes (Article) PDFJagan ReddyNoch keine Bewertungen
- Collocation SDokument2 SeitenCollocation SpatykcNoch keine Bewertungen
- Resume de José CarrasquilloDokument2 SeitenResume de José CarrasquilloJosé A. CarrasquilloNoch keine Bewertungen
- DR Ranjith CV PDFDokument4 SeitenDR Ranjith CV PDFRanjith ArNoch keine Bewertungen
- Impact of Training On The Performance of Employeees in The Public Sector - A Case Study of MoWTDokument56 SeitenImpact of Training On The Performance of Employeees in The Public Sector - A Case Study of MoWTJJINGO ISAAC100% (2)
- Quiles Jonathan Assessment SADDokument3 SeitenQuiles Jonathan Assessment SADJonathan Quiles100% (1)
- Intermittent FastingDokument5 SeitenIntermittent FastingIrfan KaSSimNoch keine Bewertungen
- Portfolio Division ListDokument12 SeitenPortfolio Division ListRosman DrahmanNoch keine Bewertungen
- Bruce Conner Catalogue PDFDokument384 SeitenBruce Conner Catalogue PDFDanut Radu SorinNoch keine Bewertungen