Das könnte Ihnen auch gefallen
- Riverhead Town Proposed Battery Energy Storage CodeDokument10 SeitenRiverhead Town Proposed Battery Energy Storage CodeRiverheadLOCALNoch keine Bewertungen
- Riverhead Budget Presentation March 22, 2022Dokument14 SeitenRiverhead Budget Presentation March 22, 2022RiverheadLOCALNoch keine Bewertungen
- 2022 - 03 - 16 - EPCAL Resolution & Letter AgreementDokument9 Seiten2022 - 03 - 16 - EPCAL Resolution & Letter AgreementRiverheadLOCALNoch keine Bewertungen
- Draft Scope Riverhead Logistics CenterDokument20 SeitenDraft Scope Riverhead Logistics CenterRiverheadLOCALNoch keine Bewertungen
- RXR/GGV Qualified & Eligible Documents (Final 09.26.22)Dokument23 SeitenRXR/GGV Qualified & Eligible Documents (Final 09.26.22)RiverheadLOCALNoch keine Bewertungen
- N.Y. Downtown Revitalization Initiative Round Five GuidebookDokument38 SeitenN.Y. Downtown Revitalization Initiative Round Five GuidebookRiverheadLOCALNoch keine Bewertungen
- Riverhead Town Board Comprehensive Plan Status Discussion Feb. 17, 2022Dokument30 SeitenRiverhead Town Board Comprehensive Plan Status Discussion Feb. 17, 2022RiverheadLOCALNoch keine Bewertungen
- Robert E. KernDokument3 SeitenRobert E. KernRiverheadLOCALNoch keine Bewertungen
- Kenneth RothwellDokument5 SeitenKenneth RothwellRiverheadLOCALNoch keine Bewertungen
- Yvette AguiarDokument10 SeitenYvette AguiarRiverheadLOCALNoch keine Bewertungen
- Turtles of New York StateDokument2 SeitenTurtles of New York StateRiverheadLOCALNoch keine Bewertungen
- AKRF Public Outreach Report AttachmentsDokument126 SeitenAKRF Public Outreach Report AttachmentsRiverheadLOCALNoch keine Bewertungen
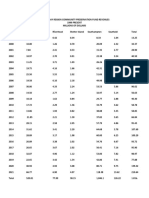
- Peconic Bay Region Community Preservation Fund Revenues 1999-2021Dokument1 SeitePeconic Bay Region Community Preservation Fund Revenues 1999-2021RiverheadLOCALNoch keine Bewertungen
- Evelyn Hobson-Womack Campaign Finance DisclosureDokument3 SeitenEvelyn Hobson-Womack Campaign Finance DisclosureRiverheadLOCALNoch keine Bewertungen
- Catherine KentDokument7 SeitenCatherine KentRiverheadLOCALNoch keine Bewertungen
- Aguiar-Kent Campaign Finance Report 32-Day Pre GeneralDokument2 SeitenAguiar-Kent Campaign Finance Report 32-Day Pre GeneralRiverheadLOCALNoch keine Bewertungen
- Riverhead Town Police Monthly Report July 2021Dokument6 SeitenRiverhead Town Police Monthly Report July 2021RiverheadLOCALNoch keine Bewertungen
- Juan Micieli-MartinezDokument3 SeitenJuan Micieli-MartinezRiverheadLOCALNoch keine Bewertungen
- 2021 General Election - Suffolk County Sample Ballot BookletDokument154 Seiten2021 General Election - Suffolk County Sample Ballot BookletRiverheadLOCALNoch keine Bewertungen
- Old Steeple Church Time CapsuleDokument4 SeitenOld Steeple Church Time CapsuleRiverheadLOCALNoch keine Bewertungen
- Riverhead Town Police Report, August 2021Dokument6 SeitenRiverhead Town Police Report, August 2021RiverheadLOCALNoch keine Bewertungen
- League of Women Voters of NYS 2021 Voters Guide: Ballot PropositionsDokument2 SeitenLeague of Women Voters of NYS 2021 Voters Guide: Ballot PropositionsRiverheadLOCAL67% (3)
- Riverhead Police Reform Plan - FinalDokument96 SeitenRiverhead Police Reform Plan - FinalRiverheadLOCALNoch keine Bewertungen
- Riverhead Town Marijuana SurveyDokument44 SeitenRiverhead Town Marijuana SurveyRiverheadLOCALNoch keine Bewertungen
- "The Case of The DIsappering Landfill, or To Mine or Not To Mine" by Carl E. Fritz JR., PEDokument10 Seiten"The Case of The DIsappering Landfill, or To Mine or Not To Mine" by Carl E. Fritz JR., PERiverheadLOCALNoch keine Bewertungen
- Riverhead Town State of Emergency Order Issued May 12, 2021Dokument3 SeitenRiverhead Town State of Emergency Order Issued May 12, 2021RiverheadLOCAL100% (1)
- Town of Southampton Police Reform PlanDokument308 SeitenTown of Southampton Police Reform PlanRiverheadLOCALNoch keine Bewertungen
- 2021-2022 Proposed Budget SummaryDokument2 Seiten2021-2022 Proposed Budget SummaryRiverheadLOCALNoch keine Bewertungen
- Town of Riverhead Draft Solid Waste Management PlanDokument73 SeitenTown of Riverhead Draft Solid Waste Management PlanRiverheadLOCALNoch keine Bewertungen
- Town of Riverhead Railroad Street TOD RedevelopmentDokument54 SeitenTown of Riverhead Railroad Street TOD RedevelopmentRiverheadLOCALNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Improvement of The Qualityof Drug Dependence Treatment Programs in SkopjeDokument68 SeitenImprovement of The Qualityof Drug Dependence Treatment Programs in SkopjeVanja DimitrievskiNoch keine Bewertungen
- Harm Reduction StudyDokument26 SeitenHarm Reduction StudyJeff MorrisNoch keine Bewertungen
- Arero Primary Hospital Pain MGT ProtocolDokument9 SeitenArero Primary Hospital Pain MGT Protocolsami ketemaNoch keine Bewertungen
- The Epidemic of Opioids in AmericaDokument13 SeitenThe Epidemic of Opioids in AmericaAliza SaddalNoch keine Bewertungen
- Drug Policy International Journal 2015Dokument48 SeitenDrug Policy International Journal 2015Thancho LinnNoch keine Bewertungen
- Nursing Writing PDFDokument42 SeitenNursing Writing PDFRyu Tse50% (2)
- substanceuseAPA PDFDokument130 SeitensubstanceuseAPA PDFAušrinė RadišauskaitėNoch keine Bewertungen
- Substance Use and Addictive DisordersDokument11 SeitenSubstance Use and Addictive Disordersrichmarkconag1100% (2)
- 1 s2.0 S1524904220302290 MainDokument11 Seiten1 s2.0 S1524904220302290 MainMuh.Anugrah GemilangNoch keine Bewertungen
- Nursing Research Paper - Opioid Use in AdolescentsDokument13 SeitenNursing Research Paper - Opioid Use in Adolescentsapi-608044542Noch keine Bewertungen
- Hepatitis B, Hepatitis C and Hiv Among Drug Users in Methadone Maintenance Treatment: Prevalence, Doses, Treatment ComplianceDokument7 SeitenHepatitis B, Hepatitis C and Hiv Among Drug Users in Methadone Maintenance Treatment: Prevalence, Doses, Treatment ComplianceIJAR JOURNALNoch keine Bewertungen
- KANCHANDokument20 SeitenKANCHANAbdulrasheed BashirNoch keine Bewertungen
- Aggressive Drivers EssayDokument57 SeitenAggressive Drivers Essayb725c62j100% (2)
- Therapeutic Communities Research ReportDokument25 SeitenTherapeutic Communities Research ReportMentari Prima OktavianiNoch keine Bewertungen
- 10 Kinds of Drug AbuseDokument10 Seiten10 Kinds of Drug AbuseJennifer Piloton CañeteNoch keine Bewertungen
- WalshcDokument26 SeitenWalshcapi-530445129Noch keine Bewertungen
- Mentalt Health 6-116Dokument16 SeitenMentalt Health 6-116Osama NasrNoch keine Bewertungen
- Monroe County 2023 BudgetDokument3 SeitenMonroe County 2023 BudgetKeegan TrunickNoch keine Bewertungen
- Commission On Combating Synthetic Opioid Trafficking: Final ReportDokument148 SeitenCommission On Combating Synthetic Opioid Trafficking: Final ReportMarco Antonio Del Toral MNoch keine Bewertungen
- Managing Opioid Withdrawal With BuprenorphineDokument7 SeitenManaging Opioid Withdrawal With BuprenorphineAgata KurniawatyNoch keine Bewertungen
- RTIReport RemovingPriorAuthDokument14 SeitenRTIReport RemovingPriorAuthBethanyNoch keine Bewertungen
- Drugs Dilemmas and ChoicesDokument304 SeitenDrugs Dilemmas and ChoicesClément JanequinNoch keine Bewertungen
- Pain and Psychology-A Reciprocal Relationship - FullDokument8 SeitenPain and Psychology-A Reciprocal Relationship - FullgetupNoch keine Bewertungen
- Pain Management Opioids SummariesDokument55 SeitenPain Management Opioids SummariesPeter KhanhNoch keine Bewertungen
- Evon Medics, LLC Has Been Awarded $1.7 Million Grant For The Evaluation of Its Medical Device For The Treatment of Opioid Use DisorderDokument2 SeitenEvon Medics, LLC Has Been Awarded $1.7 Million Grant For The Evaluation of Its Medical Device For The Treatment of Opioid Use DisorderPR.comNoch keine Bewertungen
- Should Drug Users Should Be Punish or HelpDokument25 SeitenShould Drug Users Should Be Punish or HelpMaria Sandara PatajoNoch keine Bewertungen
- Study Guide #3 (20 Points)Dokument4 SeitenStudy Guide #3 (20 Points)vanessa solanoNoch keine Bewertungen
- Bullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Dokument15 SeitenBullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Jhaylord mendozaNoch keine Bewertungen
- OVSJG 2022 Performance Oversight Hearing TestimonyDokument9 SeitenOVSJG 2022 Performance Oversight Hearing TestimonyCami MondeauxNoch keine Bewertungen
- TR 023Dokument39 SeitenTR 023Patrick PerezNoch keine Bewertungen