Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Ti Whites CountermeasureDokument60 SeitenTi Whites CountermeasureHRC100% (3)
- HCMI - HF - Generator - X-RAY GENERATOR - Service - Manual PDFDokument139 SeitenHCMI - HF - Generator - X-RAY GENERATOR - Service - Manual PDFchaparal93% (15)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
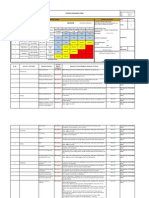
- 25-Risk Assessment For Fabrication & NDT During Night ShiftDokument2 Seiten25-Risk Assessment For Fabrication & NDT During Night Shiftgulryz84100% (9)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- RHS Exam OutlineDokument10 SeitenRHS Exam Outlinefree booksNoch keine Bewertungen
- HF50-R System12.9 PDFDokument24 SeitenHF50-R System12.9 PDFmarius vasile100% (1)
- Radiation Safety QuizDokument4 SeitenRadiation Safety QuizMaja JovanovicNoch keine Bewertungen
- Phantom: Portable X-Ray System Installation, Operation & Service ManualDokument151 SeitenPhantom: Portable X-Ray System Installation, Operation & Service ManualPepe GarciaNoch keine Bewertungen
- CRH Radiology Policies and ProceduresDokument60 SeitenCRH Radiology Policies and ProceduresAbdul Saeed Shah100% (1)
- Radiation Safety Course Powerpoint PresentationDokument59 SeitenRadiation Safety Course Powerpoint PresentationJayesh100% (1)
- 500 960 User Guide XLt797Z V5.2Dokument185 Seiten500 960 User Guide XLt797Z V5.2agooNoch keine Bewertungen
- MCQDokument3 SeitenMCQhanghouse8244Noch keine Bewertungen
- 3 RPIIDesignGuideandShielding PDFDokument112 Seiten3 RPIIDesignGuideandShielding PDFAndara BaroldusNoch keine Bewertungen
- Lessons Learned-Nuclear Gauge002Dokument66 SeitenLessons Learned-Nuclear Gauge002Michael Murillo BaraquioNoch keine Bewertungen
- Radiography Curriculum Analysis GridDokument6 SeitenRadiography Curriculum Analysis GridMostafa AbdelrahmanNoch keine Bewertungen
- 1.HF-525Plus VET (32kW, 400ma, 230Vor110V, XR5)Dokument207 Seiten1.HF-525Plus VET (32kW, 400ma, 230Vor110V, XR5)fortroniNoch keine Bewertungen
- IEC Code List (Incomplete)Dokument28 SeitenIEC Code List (Incomplete)LyunlyunNoch keine Bewertungen
- IBA Electrometer SetupDokument3 SeitenIBA Electrometer Setupamilcarla2Noch keine Bewertungen
- Point and Line SourceDokument41 SeitenPoint and Line SourceNomanNoch keine Bewertungen
- Radiation ApplicationAERBausOct2010Dokument94 SeitenRadiation ApplicationAERBausOct2010Vallabh SinghNoch keine Bewertungen
- Gallium-67 (Ga) : Physical DataDokument3 SeitenGallium-67 (Ga) : Physical DataCarlos CadavidNoch keine Bewertungen
- ThermocoupleDokument8 SeitenThermocoupleGustavo Palacios100% (1)
- Rev5 (User's Manual)Dokument53 SeitenRev5 (User's Manual)Eleanor Lou100% (1)
- Pub1663 WebDokument450 SeitenPub1663 WebYolanda HokerNoch keine Bewertungen
- 08 Lessons Learned (Industry)Dokument77 Seiten08 Lessons Learned (Industry)Michael Murillo BaraquioNoch keine Bewertungen
- 443 FullDokument8 Seiten443 FullNadya PurwantyNoch keine Bewertungen
- NOMAD MD Manual PDFDokument48 SeitenNOMAD MD Manual PDFJoe ChengNoch keine Bewertungen
- Tanzania Atomic Energy Commission: (Official Government Body Responsible For Atomic Energy Matters)Dokument7 SeitenTanzania Atomic Energy Commission: (Official Government Body Responsible For Atomic Energy Matters)abdalahkileoNoch keine Bewertungen
- Medical PhyscisDokument11 SeitenMedical PhyscisHadia NazirNoch keine Bewertungen
- Profil Paparan Radiasi Instalasi Radiologi - Dwi RochmayantiDokument5 SeitenProfil Paparan Radiasi Instalasi Radiologi - Dwi RochmayantiFadila Nur'AeniNoch keine Bewertungen
- Nuclear Engineering and Technology: Experimental Investigation of Clay Fly Ash Bricks For Gamma-Ray ShieldingDokument7 SeitenNuclear Engineering and Technology: Experimental Investigation of Clay Fly Ash Bricks For Gamma-Ray ShieldingInzimam Ul haqNoch keine Bewertungen