Das könnte Ihnen auch gefallen
- Blood Coagulation and FibrinolysisDokument63 SeitenBlood Coagulation and FibrinolysisNora AboshanadyNoch keine Bewertungen
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Von EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Noch keine Bewertungen
- Rigging TechniquesDokument27 SeitenRigging TechniquesDeepak ShettyNoch keine Bewertungen
- No Sweat - Chapter 2: Escape The Vicious Cycle of FailureDokument27 SeitenNo Sweat - Chapter 2: Escape The Vicious Cycle of FailureAMACOM, Publishing Division of the American Management AssociationNoch keine Bewertungen
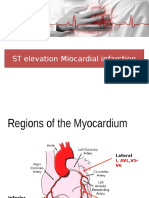
- ST Elevation Miocardial InfarctionDokument31 SeitenST Elevation Miocardial InfarctionNur Kurnia Putri Halim100% (1)
- XareltoDokument2 SeitenXareltoMichael KuzbytNoch keine Bewertungen
- Drug StudyDokument10 SeitenDrug StudyFranco ObedozaNoch keine Bewertungen
- Chemo MedsDokument17 SeitenChemo MedsSophia Smartz100% (1)
- Pharmacology Emergency DrugsDokument5 SeitenPharmacology Emergency DrugsAce RegellanaNoch keine Bewertungen
- UWORLDNCLEXreview2021 090Dokument100 SeitenUWORLDNCLEXreview2021 090lilchibaby3161100% (1)
- Alert Medical Series: Emergency Medicine Alert I, II, IIIVon EverandAlert Medical Series: Emergency Medicine Alert I, II, IIINoch keine Bewertungen
- Employee Benefits India PDFDokument2 SeitenEmployee Benefits India PDFshahidki31100% (1)
- Iman Tavassoly CVDokument6 SeitenIman Tavassoly CVGladis HutahaeanNoch keine Bewertungen
- Mmda V Concerned Citizens of Manila Bay (GR No 171947) DigestDokument2 SeitenMmda V Concerned Citizens of Manila Bay (GR No 171947) DigestJose Ramon Ampil83% (6)
- ASSIGNMENT AND ACTIVITIES in Contemp FinalDokument14 SeitenASSIGNMENT AND ACTIVITIES in Contemp FinalalmahairaNoch keine Bewertungen
- UWORLDNCLEXreview2021 Watermarked PDFDokument100 SeitenUWORLDNCLEXreview2021 Watermarked PDFashley100% (1)
- AnticoagulantDokument15 SeitenAnticoagulantMaine AsuncionNoch keine Bewertungen
- Konika 7045 Service Manual PDFDokument313 SeitenKonika 7045 Service Manual PDFleo visaNoch keine Bewertungen
- Drug StudyDokument4 SeitenDrug StudySharwen_R_Rome_5572Noch keine Bewertungen
- FebuxostatDokument2 SeitenFebuxostatJoshua Pascasio100% (1)
- Qtern 84413Dokument19 SeitenQtern 84413Manoj KaluvakotaNoch keine Bewertungen
- Aspirin 75mg Tablets: 1. Name of The Medicinal Product 2. Qualitative and Quantitative CompositionDokument11 SeitenAspirin 75mg Tablets: 1. Name of The Medicinal Product 2. Qualitative and Quantitative CompositionSunil SewakNoch keine Bewertungen
- ATORVASTATINDokument4 SeitenATORVASTATINeshikaNoch keine Bewertungen
- Medication ListDokument16 SeitenMedication ListxNoch keine Bewertungen
- DrugDokument13 SeitenDrugkhesler BacallaNoch keine Bewertungen
- AllopurinolDokument3 SeitenAllopurinolapi-3797941100% (1)
- Patient AssignmentDokument6 SeitenPatient AssignmentRj MagalingNoch keine Bewertungen
- PlasmanateDokument4 SeitenPlasmanateroelNoch keine Bewertungen
- Drug Card PradaxaDokument2 SeitenDrug Card PradaxaBenNoch keine Bewertungen
- Coronary Heart Disease With AsthmaDokument31 SeitenCoronary Heart Disease With AsthmaEf LablaNoch keine Bewertungen
- Perindopril ErbumineDokument8 SeitenPerindopril ErbumineYanna Habib-MangotaraNoch keine Bewertungen
- Drug Study - ERDokument10 SeitenDrug Study - ERbabiNoch keine Bewertungen
- Ramipril Drug StudyDokument3 SeitenRamipril Drug StudyCheezy Bread0% (1)
- Ipratropium BromideDokument20 SeitenIpratropium BromideAngelique Ramos PascuaNoch keine Bewertungen
- DR (High Risk) Drug Study and ReadingDokument5 SeitenDR (High Risk) Drug Study and ReadingDea Sabelle CastroNoch keine Bewertungen
- Metformin: Dosing & UsesDokument8 SeitenMetformin: Dosing & UsesMaria Alejandra Siachoque JaraNoch keine Bewertungen
- Summary of Product CharacteristicsDokument8 SeitenSummary of Product CharacteristicsKirubakaranNoch keine Bewertungen
- Medication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Dokument43 SeitenMedication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Kath Rubio0% (1)
- Drug StudyDokument5 SeitenDrug Studyjanelle123 toribioNoch keine Bewertungen
- Allopurinol Drug Study WWW RNpedia ComDokument9 SeitenAllopurinol Drug Study WWW RNpedia ComifyNoch keine Bewertungen
- Ify Drug StudiesDokument15 SeitenIfy Drug StudiesifyNoch keine Bewertungen
- Indications: Details With Side EffectsDokument5 SeitenIndications: Details With Side EffectsJillian HernandezNoch keine Bewertungen
- AtorvastatinDokument7 SeitenAtorvastatinKrima PatelNoch keine Bewertungen
- Aggrastat: Name of MedicineDokument10 SeitenAggrastat: Name of MedicineCamilo VallejoNoch keine Bewertungen
- WarfarinDokument4 SeitenWarfarinekramNoch keine Bewertungen
- AtorvastatinDokument5 SeitenAtorvastatinmehnoor kaurNoch keine Bewertungen
- Esophageal Varices: Medication HistoryDokument4 SeitenEsophageal Varices: Medication HistoryNeil Patrick PasuquinNoch keine Bewertungen
- VASCORDokument2 SeitenVASCORmoasrisNoch keine Bewertungen
- Drug StudyDokument8 SeitenDrug StudyChristine MatasNoch keine Bewertungen
- As Pi LetDokument7 SeitenAs Pi Letianecunar100% (1)
- Duplicate Therapy Issues: This Product Contains Acetaminophen, Which May Be A ComponentDokument15 SeitenDuplicate Therapy Issues: This Product Contains Acetaminophen, Which May Be A ComponentDevi KusumaNoch keine Bewertungen
- Atacor SPCDokument9 SeitenAtacor SPCRannia1Noch keine Bewertungen
- Drug Study CCUDokument5 SeitenDrug Study CCUKrishna Faith P. DelaraNoch keine Bewertungen
- Tylenol (Acetaminophen)Dokument2 SeitenTylenol (Acetaminophen)gagandipkSNoch keine Bewertungen
- Cardiovascular Disease and Risk ManagementDokument25 SeitenCardiovascular Disease and Risk ManagementYhang L TamaNoch keine Bewertungen
- Icu Drug StudyDokument7 SeitenIcu Drug StudyHazel Palomares100% (1)
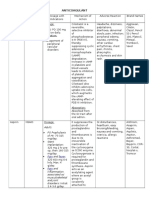
- Ix. Pharmacologic Management Brand Name Classification Indication Mechanism of Action Dosage and Frequency Adverse Reactions Nursing ConsiderationDokument21 SeitenIx. Pharmacologic Management Brand Name Classification Indication Mechanism of Action Dosage and Frequency Adverse Reactions Nursing ConsiderationDizerine Mirafuentes RolidaNoch keine Bewertungen
- XareltoDokument2 SeitenXareltoMichael Kuzbyt100% (1)
- Spironolactone: Generic Name Brand Name ClassificationDokument5 SeitenSpironolactone: Generic Name Brand Name ClassificationShermalyn SalahuddinNoch keine Bewertungen
- Anti Platelets Agents: Dr. Sachana KC 1 Year Resident Department of AnesthesiaDokument61 SeitenAnti Platelets Agents: Dr. Sachana KC 1 Year Resident Department of AnesthesiaKshitizma GiriNoch keine Bewertungen
- Drug Study Ko ToDokument4 SeitenDrug Study Ko ToGian Carlo FernandezNoch keine Bewertungen
- AllopurinolDokument48 SeitenAllopurinolFarha Elein KukihiNoch keine Bewertungen
- Narrow Therapeutic Range ExpandedDokument3 SeitenNarrow Therapeutic Range ExpandedHaleema Sadia KhanNoch keine Bewertungen
- Aspilets ECDokument5 SeitenAspilets ECJerry SerapionNoch keine Bewertungen
- Drugstudy For ElderlyDokument14 SeitenDrugstudy For ElderlyJenniferP.BarrosoNoch keine Bewertungen
- Obesity and Overweight Who FactsDokument6 SeitenObesity and Overweight Who FactsNur Kurnia Putri HalimNoch keine Bewertungen
- STEMI Anteriorseptal 121015Dokument37 SeitenSTEMI Anteriorseptal 121015Nur Kurnia Putri HalimNoch keine Bewertungen
- Gambaran Umum USG Prof BA Mar14Dokument47 SeitenGambaran Umum USG Prof BA Mar14Nur Kurnia Putri HalimNoch keine Bewertungen
- Daftar Pustaka PJTDokument1 SeiteDaftar Pustaka PJTNur Kurnia Putri HalimNoch keine Bewertungen
- Family-Based Therapy For Adolescents With Bulimia NervosaDokument15 SeitenFamily-Based Therapy For Adolescents With Bulimia NervosaNur Kurnia Putri HalimNoch keine Bewertungen
- Irradiated Foods 2003 PDFDokument52 SeitenIrradiated Foods 2003 PDFDiana BratuNoch keine Bewertungen
- BAYBAY AwardsDokument63 SeitenBAYBAY AwardsClennil Palmes SustraidoNoch keine Bewertungen
- Table Saw Safety FinalDokument24 SeitenTable Saw Safety Finalvolatileyasser100% (1)
- Applying A Feminist Lens To Indias Foreign Policy A Compendium of EssaysDokument124 SeitenApplying A Feminist Lens To Indias Foreign Policy A Compendium of EssaysRasced AliNoch keine Bewertungen
- Aspiracion Destornillador Implanto Roa-V1-Id1018Dokument3 SeitenAspiracion Destornillador Implanto Roa-V1-Id1018CesarAmorotoNoch keine Bewertungen
- A Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDokument11 SeitenA Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDinesh babuNoch keine Bewertungen
- Ijc Heart & Vasculature: SciencedirectDokument8 SeitenIjc Heart & Vasculature: SciencedirectFerdi YuanNoch keine Bewertungen
- Share FORM 10 - Workplace Application Evaluation ToolDokument3 SeitenShare FORM 10 - Workplace Application Evaluation ToolRocel Ann CarantoNoch keine Bewertungen
- NDEPDokument5 SeitenNDEPjoeNoch keine Bewertungen
- Taylan Competency NeedsDokument32 SeitenTaylan Competency NeedsLovejoice Cha NnelNoch keine Bewertungen
- Progressive Addition Lens Design and The Short of Stature (Shan-Yu, S.)Dokument3 SeitenProgressive Addition Lens Design and The Short of Stature (Shan-Yu, S.)Valentina PereaNoch keine Bewertungen
- Exam Table For Shoulder and ElbowDokument17 SeitenExam Table For Shoulder and ElbowLouie OkayNoch keine Bewertungen
- Quantitative Analysis of Lead, Cadmium and Chromium Found in Selected Fish Marketed in Metro Manila, PhilippinesDokument6 SeitenQuantitative Analysis of Lead, Cadmium and Chromium Found in Selected Fish Marketed in Metro Manila, PhilippinesMstkasrNoch keine Bewertungen
- Walk or Cycle For 'A Happier Commute': BBC Learning English Words in The NewsDokument2 SeitenWalk or Cycle For 'A Happier Commute': BBC Learning English Words in The NewsCaio Augusto Takaki UechiNoch keine Bewertungen
- Liver UpdateDokument16 SeitenLiver UpdateyaniNoch keine Bewertungen
- Biological Molecules 2 QPDokument12 SeitenBiological Molecules 2 QPApdiweli AliNoch keine Bewertungen
- Ejsr Vol 97 Issue 1 159 171Dokument171 SeitenEjsr Vol 97 Issue 1 159 171Raja ChandruNoch keine Bewertungen
- Tinnitus Today September 1986 Vol 11, No 3Dokument8 SeitenTinnitus Today September 1986 Vol 11, No 3American Tinnitus AssociationNoch keine Bewertungen
- Wireless Patch Sensor For Remote Monitoring of Heart Rate, RESPIRASI and FALLDokument4 SeitenWireless Patch Sensor For Remote Monitoring of Heart Rate, RESPIRASI and FALLAgung Tri SutrisnoNoch keine Bewertungen
- Psychometric Properties of The Consensus Sleep Diary in Those With Insomnia DisorderDokument19 SeitenPsychometric Properties of The Consensus Sleep Diary in Those With Insomnia DisorderMondlTNoch keine Bewertungen
- CPRDokument45 SeitenCPRJames Elwood DoyolaNoch keine Bewertungen
- Proposal For The BoosterDokument5 SeitenProposal For The BoosterraziNoch keine Bewertungen
- Moods, Environments, SituationsDokument9 SeitenMoods, Environments, SituationsHery MuhendraNoch keine Bewertungen