Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The ESC Textbook of Cardiovascular Medicine PDFDokument1.109 SeitenThe ESC Textbook of Cardiovascular Medicine PDFjyothi100% (4)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Nursing Care Plan 6 Impaired Gas ExchangeDokument9 SeitenNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
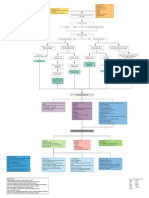
- Myocardial Infarction With CABG Concept MapDokument1 SeiteMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Tutorial 9 PDFDokument6 SeitenTutorial 9 PDFPututWisnuNugrohoNoch keine Bewertungen
- PACU Monitoring Sheet - RR Record - SCT-CONDokument4 SeitenPACU Monitoring Sheet - RR Record - SCT-CONFitz JaminitNoch keine Bewertungen
- Pregabalina Vs Gabapentina SuplementoDokument7 SeitenPregabalina Vs Gabapentina SuplementoCh RoNoch keine Bewertungen
- DeliriumEdCards PDFDokument5 SeitenDeliriumEdCards PDFCh RoNoch keine Bewertungen
- Hydroxychloroquine Final DOI IJAADokument24 SeitenHydroxychloroquine Final DOI IJAAgervais100% (4)
- Anticoagulan TherpayDokument17 SeitenAnticoagulan TherpayCh RoNoch keine Bewertungen
- Brat Er 2011Dokument12 SeitenBrat Er 2011Ch RoNoch keine Bewertungen
- Acceso IntraoseoDokument5 SeitenAcceso IntraoseoCh RoNoch keine Bewertungen
- Nej MV CM 1105237Dokument5 SeitenNej MV CM 1105237Marco Vinicio IGNoch keine Bewertungen
- ArtrocentesisDokument3 SeitenArtrocentesisFiorella BolivarNoch keine Bewertungen
- Rules of Five Primer On Clinical Acid-Base Problem SolvingDokument41 SeitenRules of Five Primer On Clinical Acid-Base Problem SolvingCh RoNoch keine Bewertungen
- PelvisDokument12 SeitenPelvisCh RoNoch keine Bewertungen
- The "Epic" Challenge of Optimizing Antimicrobial Stewardship: The Role of Electronic Medical Records and TechnologyDokument9 SeitenThe "Epic" Challenge of Optimizing Antimicrobial Stewardship: The Role of Electronic Medical Records and TechnologyMr XNoch keine Bewertungen
- Evaluasi Penatalaksanaan Prolanis Di Puskesmas Kota BengkuluDokument11 SeitenEvaluasi Penatalaksanaan Prolanis Di Puskesmas Kota Bengkulunanasila02Noch keine Bewertungen
- Student'S Copy Please Do Not DuplicateDokument134 SeitenStudent'S Copy Please Do Not DuplicateChn ypNoch keine Bewertungen
- Cleansing and Moist Greg Goodman 2009Dokument1 SeiteCleansing and Moist Greg Goodman 2009Prajnamita Manindhya El FarahNoch keine Bewertungen
- First Aid Quiz IDokument32 SeitenFirst Aid Quiz Ianon_617170800Noch keine Bewertungen
- Shah - Cancer of The Head and Neck PDFDokument12 SeitenShah - Cancer of The Head and Neck PDFElizabetha SalzcenNoch keine Bewertungen
- Burning Mouth SyndromeDokument40 SeitenBurning Mouth SyndromeSuci Sylvana HrpNoch keine Bewertungen
- Drug in PregnancyDokument49 SeitenDrug in PregnancyGarry B GunawanNoch keine Bewertungen
- Information Revolution Roadmap - Final - April - 2016-1Dokument62 SeitenInformation Revolution Roadmap - Final - April - 2016-1Amenti TekaNoch keine Bewertungen
- Activity 8 - 5 Issues in The PhilippinesDokument3 SeitenActivity 8 - 5 Issues in The PhilippinesChristel Mae BoseoNoch keine Bewertungen
- The International Journal of Periodontics & Restorative DentistryDokument10 SeitenThe International Journal of Periodontics & Restorative DentistryAna Maria Montoya GomezNoch keine Bewertungen
- TB Screening Form For TAMUDokument1 SeiteTB Screening Form For TAMUmandar0072100% (1)
- Repaske 2008Dokument2 SeitenRepaske 2008Esteban Martin Chiotti KaneshimaNoch keine Bewertungen
- Intervenciones en Dermatitis Atópica CaninaDokument16 SeitenIntervenciones en Dermatitis Atópica CaninaMaka.ibanezNoch keine Bewertungen
- Clinico-Pathological Conference: Presented by The Department of Internal MedicineDokument3 SeitenClinico-Pathological Conference: Presented by The Department of Internal MedicineCloudy ClaudNoch keine Bewertungen
- Dr. Rachmat Gunadi - Vitamin D - Autoimmune Prodia Final PDFDokument38 SeitenDr. Rachmat Gunadi - Vitamin D - Autoimmune Prodia Final PDFNururrohmahNoch keine Bewertungen
- Chapter 15 - A Safe Diagnostic Strategy: The Basic ModelDokument13 SeitenChapter 15 - A Safe Diagnostic Strategy: The Basic Modelprofarmah6150Noch keine Bewertungen
- 4564 2934 p436 Pages Deleted EditedDokument4 Seiten4564 2934 p436 Pages Deleted EditedHaniNoch keine Bewertungen
- Principles of Aseptic TechniqueDokument5 SeitenPrinciples of Aseptic TechniqueNicole Audrey JoaquinNoch keine Bewertungen
- Breast Self ExaminationDokument40 SeitenBreast Self ExaminationPrince Rener Velasco PeraNoch keine Bewertungen
- Siraj Sir Artical IjprdDokument11 SeitenSiraj Sir Artical IjprdmwdhtirahNoch keine Bewertungen
- IARC Monograph - Carcinogen PDFDokument498 SeitenIARC Monograph - Carcinogen PDFEma KusumaNoch keine Bewertungen
- Ophthalmia NeonatorumDokument17 SeitenOphthalmia NeonatorumIndranil DuttaNoch keine Bewertungen
- Immunopotentiation: Immunopotentiation Can Be Defined As The ProcessDokument67 SeitenImmunopotentiation: Immunopotentiation Can Be Defined As The ProcesssamyNoch keine Bewertungen
- Osteomyelitis: Mariamawit B Dbu, College of MedicineDokument34 SeitenOsteomyelitis: Mariamawit B Dbu, College of MedicinedenekeNoch keine Bewertungen