Das könnte Ihnen auch gefallen
- Job Description / Competency Profile: Job Title Payband/Grade Directorate Job Description ReferenceDokument5 SeitenJob Description / Competency Profile: Job Title Payband/Grade Directorate Job Description ReferencenasimhsNoch keine Bewertungen
- Acute Kidney Injury: Chapter ContentsDokument22 SeitenAcute Kidney Injury: Chapter ContentsnasimhsNoch keine Bewertungen
- PT - and NursesDokument7 SeitenPT - and NursesnasimhsNoch keine Bewertungen
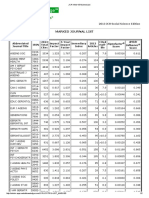
- Marked Journal List: 2013 JCR Social Science EditionDokument2 SeitenMarked Journal List: 2013 JCR Social Science EditionnasimhsNoch keine Bewertungen
- Performing An A-G Patient Assessment: A Step-By-Step GuideDokument3 SeitenPerforming An A-G Patient Assessment: A Step-By-Step GuidenasimhsNoch keine Bewertungen
- 14.4 MSDokument14 Seiten14.4 MSnasimhsNoch keine Bewertungen
- Acute Decompensated Heart Failure: A Study of Nursing CareDokument12 SeitenAcute Decompensated Heart Failure: A Study of Nursing CarenasimhsNoch keine Bewertungen
- Using A Systematic Approach To Assess An Acutely Unwell Patient With Catatonia: A Case StudyDokument9 SeitenUsing A Systematic Approach To Assess An Acutely Unwell Patient With Catatonia: A Case StudynasimhsNoch keine Bewertungen
- Acute Kidney Injury: Mark BevanDokument42 SeitenAcute Kidney Injury: Mark BevannasimhsNoch keine Bewertungen
- Accelerated Idioventricular RhythmDokument4 SeitenAccelerated Idioventricular RhythmnasimhsNoch keine Bewertungen
- Marked Journal List: 2013 JCR Social Science EditionDokument2 SeitenMarked Journal List: 2013 JCR Social Science EditionnasimhsNoch keine Bewertungen
- Marked Journal List: 2013 JCR Social Science EditionDokument2 SeitenMarked Journal List: 2013 JCR Social Science EditionnasimhsNoch keine Bewertungen
- Which of The Following Statements About The Human Nervous System Is True?Dokument12 SeitenWhich of The Following Statements About The Human Nervous System Is True?nasimhsNoch keine Bewertungen
- Marked Journal List: 2013 JCR Social Science EditionDokument2 SeitenMarked Journal List: 2013 JCR Social Science EditionnasimhsNoch keine Bewertungen
- (IELTSMaterial - Com) 100 IELTS Speaking Part 2 Topics in 2016 & 2017 & Sample Answers PDFDokument135 Seiten(IELTSMaterial - Com) 100 IELTS Speaking Part 2 Topics in 2016 & 2017 & Sample Answers PDFUyenNoch keine Bewertungen
- Media PDFDokument21 SeitenMedia PDFlethuhaiNoch keine Bewertungen
- AirwayDokument2 SeitenAirwaynasimhsNoch keine Bewertungen
- Accelerated Idioventricular RhythmDokument4 SeitenAccelerated Idioventricular RhythmnasimhsNoch keine Bewertungen
- Role of Observational Medicine in EmergencyDokument13 SeitenRole of Observational Medicine in EmergencyazhaabazNoch keine Bewertungen
- Pharmacology Review For NursesDokument11 SeitenPharmacology Review For Nursesisabel_avancena100% (4)
- Blood TubesDokument1 SeiteBlood TubesnasimhsNoch keine Bewertungen
- Nclex Lab ValuesDokument6 SeitenNclex Lab ValuesnasimhsNoch keine Bewertungen
- Weight Box SHOTDokument1 SeiteWeight Box SHOTnasimhsNoch keine Bewertungen
- Lex-Mental HealthDokument49 SeitenLex-Mental HealthnasimhsNoch keine Bewertungen
- Pharmacology Review For NursesDokument11 SeitenPharmacology Review For Nursesisabel_avancena100% (4)
- Common Laboratory Values PDF GreenDokument11 SeitenCommon Laboratory Values PDF GreennasimhsNoch keine Bewertungen
- λεξ ψ υγειαDokument87 Seitenλεξ ψ υγειαnasimhsNoch keine Bewertungen
- OET Writing and Speaking Made Easy For NursesDokument143 SeitenOET Writing and Speaking Made Easy For NursesLiju K Oommen97% (32)
- Unexpected Transfusion blc6991p FinalDokument2 SeitenUnexpected Transfusion blc6991p FinalnasimhsNoch keine Bewertungen
- Nerve SynapseDokument2 SeitenNerve SynapsenasimhsNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Communication The Social Matrix of Psychiatry PDFDokument2 SeitenCommunication The Social Matrix of Psychiatry PDFCarol0% (2)
- A Case Study of Alcohol Dependence Syndrome With Poor Motivation and Coping Skills: A Psychosocial PerspectiveDokument4 SeitenA Case Study of Alcohol Dependence Syndrome With Poor Motivation and Coping Skills: A Psychosocial Perspectivealexandra mariaNoch keine Bewertungen
- HiDokument9 SeitenHiJed HernandezNoch keine Bewertungen
- Executive Functioning PresentationDokument55 SeitenExecutive Functioning Presentationnplattos100% (3)
- Case Study - Mental HealthDokument9 SeitenCase Study - Mental Healthapi-380891151Noch keine Bewertungen
- Our Counselling Expert BrochureDokument10 SeitenOur Counselling Expert BrochureChinu AgrawalNoch keine Bewertungen
- Safe and Healthy School Operations, Contingency Plans, and Communications PlansDokument9 SeitenSafe and Healthy School Operations, Contingency Plans, and Communications PlansRodnel MonceraNoch keine Bewertungen
- Eysecnks PErsonality Questionnaire - REvised (EPQ-R)Dokument6 SeitenEysecnks PErsonality Questionnaire - REvised (EPQ-R)BN Angel Khailochho80% (5)
- Trigger WarningsDokument2 SeitenTrigger WarningsRosieNoch keine Bewertungen
- (Mary de Young) Madness An American History of MeDokument303 Seiten(Mary de Young) Madness An American History of MeVigneshwaran Vikki100% (1)
- Planning and Design of Psychiatric FacilitiesDokument57 SeitenPlanning and Design of Psychiatric FacilitiesLyra EspirituNoch keine Bewertungen
- Anushree BallDokument3 SeitenAnushree BallSanchari NagNoch keine Bewertungen
- OpheaDokument75 SeitenOpheaapi-391714949Noch keine Bewertungen
- Main Hesse 1990 Parents Unresolved Traumatic Experiences Related To Infant Disorganized Attachment StatusDokument26 SeitenMain Hesse 1990 Parents Unresolved Traumatic Experiences Related To Infant Disorganized Attachment StatusKevin McInnes100% (4)
- VA Whistleblower Alleges Discrimination For Exposing EvidenceDokument39 SeitenVA Whistleblower Alleges Discrimination For Exposing EvidenceWKYC.comNoch keine Bewertungen
- Psychoanalytic Theories: Carl Jung (1875-1961)Dokument6 SeitenPsychoanalytic Theories: Carl Jung (1875-1961)Sean KingNoch keine Bewertungen
- 9/geriatric Depression Scale (GDS) : Clinical GerontologistDokument10 Seiten9/geriatric Depression Scale (GDS) : Clinical GerontologistTeresa GasparNoch keine Bewertungen
- Case Study On Autism Spectrum DisorderDokument8 SeitenCase Study On Autism Spectrum DisorderRaquel Cantos100% (1)
- 5 Point Framework For Community Violence ReductionDokument1 Seite5 Point Framework For Community Violence ReductionDougNoch keine Bewertungen
- Therapeutic Use of MagicDokument7 SeitenTherapeutic Use of Magicapi-355156097Noch keine Bewertungen
- Mental Health Triage Tool 2006Dokument1 SeiteMental Health Triage Tool 2006MelbourneFXNoch keine Bewertungen
- Dear Abby 8Dokument3 SeitenDear Abby 8LynnNoch keine Bewertungen
- Relationship Between Quality of Life and Social SupportDokument9 SeitenRelationship Between Quality of Life and Social SupportDragos IvanNoch keine Bewertungen
- Implicit and Self-Attributed Dependency Needs in Dependent and Histrionic Personality Disorders Bornstein 1998Dokument15 SeitenImplicit and Self-Attributed Dependency Needs in Dependent and Histrionic Personality Disorders Bornstein 1998Cualit14Noch keine Bewertungen
- Guided ImageryDokument160 SeitenGuided ImageryDunja StojkovicNoch keine Bewertungen
- EmdrDokument14 SeitenEmdrapi-506787522100% (1)
- Detailed Lesson Plan in DrugsDokument6 SeitenDetailed Lesson Plan in Drugsjerrymie100% (1)
- 1 PyromaniaDokument3 Seiten1 Pyromaniayeremias setyawanNoch keine Bewertungen
- Emotional & Behavioural Presentation Puru SirDokument18 SeitenEmotional & Behavioural Presentation Puru SirMandira DhakalNoch keine Bewertungen
- Chapter 13 EvaluationDokument20 SeitenChapter 13 EvaluationNicole JusinoNoch keine Bewertungen