Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- NZDE Civil Major Courses Lecture Guides Oct 2010Dokument40 SeitenNZDE Civil Major Courses Lecture Guides Oct 2010Mat Tjs100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- FT 231Dokument9 SeitenFT 231Mat TjsNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Teaching StrategiesDokument42 SeitenTeaching StrategiesMat TjsNoch keine Bewertungen
- Virm Light Vehicle Repair CertificationDokument134 SeitenVirm Light Vehicle Repair CertificationMat TjsNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- 2018 NZDE - CET Timetable Ver1Dokument1 Seite2018 NZDE - CET Timetable Ver1Mat TjsNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Hamilton CC Wastewater Code PDFDokument83 SeitenHamilton CC Wastewater Code PDFMat TjsNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- STEM Emphasis For Your SchoolDokument6 SeitenSTEM Emphasis For Your SchoolMat TjsNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- CCC Water Supply Overview MapDokument1 SeiteCCC Water Supply Overview MapMat TjsNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Examples From Electrical Circuits Example 1Dokument3 SeitenExamples From Electrical Circuits Example 1Mat TjsNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Wastewater HCCDokument83 SeitenWastewater HCCMat TjsNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Action ResearchDokument7 SeitenAction ResearchMat TjsNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hydrostatic Pressure Project Linked-Class Problem-Based Learning in EngineeringDokument8 SeitenHydrostatic Pressure Project Linked-Class Problem-Based Learning in EngineeringMat TjsNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Teaching For Conceptual Change PDFDokument25 SeitenTeaching For Conceptual Change PDFMat TjsNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Chapter 44 Activity and ExerciseDokument7 SeitenChapter 44 Activity and ExerciseKathleen FrugalidadNoch keine Bewertungen
- Becoming Pain Free Summit 2022 Day 3Dokument5 SeitenBecoming Pain Free Summit 2022 Day 3Paul Ioan PopescuNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Lecture 1 - Introduction To Plant AnatomyDokument62 SeitenLecture 1 - Introduction To Plant AnatomyRalph AlbertoNoch keine Bewertungen
- Inheritance 14.2Dokument6 SeitenInheritance 14.2YashodhaNoch keine Bewertungen
- Block Diagram: P552LJ Repair GuideDokument5 SeitenBlock Diagram: P552LJ Repair Guidepesce provaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Westcotts Plant Disease HandbookDokument185 SeitenWestcotts Plant Disease Handbooktira flechasNoch keine Bewertungen
- Pengaruh Pemberian Infusa Daun KemuningDokument66 SeitenPengaruh Pemberian Infusa Daun Kemuningvidianka rembulanNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Mechanisms of Perception Hearing, Touch, Smell, Taste and AttentionDokument22 SeitenMechanisms of Perception Hearing, Touch, Smell, Taste and Attentiontomiwa iluromiNoch keine Bewertungen
- 15 YRC Book of AbstractsDokument107 Seiten15 YRC Book of AbstractsJelena ZdravkovicNoch keine Bewertungen
- Filaments in Bioprocesses: Rainer Krull Thomas Bley EditorsDokument370 SeitenFilaments in Bioprocesses: Rainer Krull Thomas Bley EditorsMel Esparza0% (1)
- Presentation1 1Dokument15 SeitenPresentation1 1Manula MuthunayakeNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
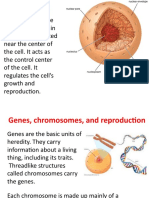
- The Parts of The Cell and Their FunctionsDokument2 SeitenThe Parts of The Cell and Their Functionsraphael100% (1)
- Current Concepts On How To Optimise Skin Needling 2020 2Dokument6 SeitenCurrent Concepts On How To Optimise Skin Needling 2020 2maat1Noch keine Bewertungen
- Microbe Report 2Dokument9 SeitenMicrobe Report 2maibmaNoch keine Bewertungen
- Anexo Norma HolandesaDokument13 SeitenAnexo Norma HolandesaThePomboNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Hema I Chapter 8 - DiffDokument67 SeitenHema I Chapter 8 - DiffderibewNoch keine Bewertungen
- Rife Morris FishbeinDokument9 SeitenRife Morris FishbeinuncoveringconsciousNoch keine Bewertungen
- Xtremely Imple: WBC 5 Part DifferentialDokument2 SeitenXtremely Imple: WBC 5 Part DifferentialSalah Al-Absi100% (1)
- SOF Level 2 NSO Class 3 PDFDokument5 SeitenSOF Level 2 NSO Class 3 PDFparesh_dhakeNoch keine Bewertungen
- LettersDokument5 SeitenLettersCarolina Rodriguez GuarinNoch keine Bewertungen
- Evs ProjectDokument3 SeitenEvs ProjectPallavi BanerjeeNoch keine Bewertungen
- Adult Development and AgingDokument44 SeitenAdult Development and AgingDiana DayenNoch keine Bewertungen
- Name of Disease: Apple ScabDokument18 SeitenName of Disease: Apple Scabapi-310125081Noch keine Bewertungen
- Understanding and Leveraging Phenotypic PlasticityDokument11 SeitenUnderstanding and Leveraging Phenotypic Plasticitysneha.921530sharmaNoch keine Bewertungen
- One Year Joint Package With AIATS For NEET 2024 - Class XII PDFDokument38 SeitenOne Year Joint Package With AIATS For NEET 2024 - Class XII PDFRishabh kumar SinghNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hemoglobin (Mass - Volume) in BloodDokument5 SeitenHemoglobin (Mass - Volume) in BloodUci Rahmawati UtamiNoch keine Bewertungen
- Catalogo Nuevo GboDokument7 SeitenCatalogo Nuevo GboCaro ErazoNoch keine Bewertungen
- WhatisResilience PDFDokument9 SeitenWhatisResilience PDFArianiNoch keine Bewertungen
- JGXP - 2011 - v15n4 - Contamination Control in The Compliance Program PDFDokument7 SeitenJGXP - 2011 - v15n4 - Contamination Control in The Compliance Program PDFNelson Alejandro FierroNoch keine Bewertungen
- Fascias y YogaDokument8 SeitenFascias y YogaJuanCarlosCernudaNoch keine Bewertungen