ORIGINAL ARTICLE
Sequelae of Septic Arthritis of the Hip in Children
A New Classification and a Review of 41 Hips
Edilson Forlin, MD, MSc, PhD* and Carlo Milani, MD, MSc, PhD
Background: The sequelae of septic arthritis of the hip in children
are diverse and represent a complex problem. A classication of the
deformities is important to plan treatment and to give prognostic
information. The radiographic main classication used provides detailed information of the deformities, but it is complicated and not
feasible to apply in young children. The authors developed a simple
and reliable method of classication and present the results of a
large series of patients.
Methods: The authors reviewed 37 children with 41 hips with
sequelae of septic arthritis of the hip. Twenty-four were male subjects,
and 13 were female subjects. Twenty-ve had the acute infection at
the neonatal period, and 16 were aged between 1 month and 3 years.
None of them received adequate treatment at the acute process:
20 hips were not treated, and the other 21 had delayed drainage (at
least 5 days after the onset of the infection). The hips were classied
into 2 groups on the basis of radiographic appearance. Hips with
sequelae grade 1 were reduced hips, with femoral head preserved
(1A) or absent (1B); hips grade 2 were dislocated hips, with the
femoral head preserved (2A) or absent (2B). There were 10 hips with
grade 1A, 11 with grade 1B, 3 with grade 2A, and 17 were grade 2B.
We compared our material and results with those presented by Choi
et al and also compared the reliability of both classication.
The criteria for satisfactory results were stability, range of motion
of 50 degrees or more of exion, a exion contraction below 20
degrees, and a painless hip.
Results: Our classication presented a greater concordance (25 of
41 hips against 7 in 41 for the Choi et al classication; P = 0.01).
Thirty-seven hips were pain-free, and 4 had occasional pain. Thirtyseven hips had a satisfactory range of motion (90.2%). Stability was
present in 29 hips (70.7%). Final results showed 24 hips classied as
satisfactory and 17 as unsatisfactory. Our material and end results
were comparable with those reported by Choi et al.
Septic arthritis of the hip developed at the newborn period
produced more severe sequelae. Hips with sequelae grade 1 have a
good prognosis. Surgical procedures in these grades were necessary
to correct acetabular dysplasia and improve congruency. Fifteen of 20
hips with sequelae grade 2 (unstable) underwent reconstruction. At a
mean follow-up of 6.9 years (range, 2.7Y11.3 years), satisfactory
results were obtained in 8 of them.
From the *Hospital Pequeno Principe, Curitiba, Pr; Hospital de Clinicas da
Universidade Federal do Parana, Curitiba, Pr; University Federal of Sao
Paulo; and Medicine School of Foundation of ABC, Sao Bernardo, Sao
Paulo, Brazil.
Study performed at Hospital Pequeno Prncipe, Curitiba, Parana, Brazil, and
Universidade Federal of Sao PauloYEscola Paulista de Medicina, Sao
Paulo, Brazil.
None of the authors received financial support for this study.
Reprints: Edilson Forlin, MD, MSc, PhD, Rua Buenos Aires, 1020, Curitiba
Pr, 80250-070 Brazil. E-mail: ediforlin@hotmail.com.
Copyright * 2008 by Lippincott Williams & Wilkins
524
Conclusions: The classication we proposed showed to be simpler
and more reliable than the classication proposed by Choi et al. It
may be useful to guide treatment and prognosis. Longer follow-up is
needed to assess the real benet of the reconstruction for unstable hips.
Level of Evidence: Therapeutic study, level IV (case series [no
control, or historic, group]).
Key Words: hip, septic joint, deformities, neonates, children
(J Pediatr Orthop 2008;28:524Y528)
elay of the diagnosis and treatment of septic arthritis of
the hip (SAH) leads to involvement and damage of structures of the joint such as articular cartilage, epiphyses, acetabulum, proximal femur metaphysic, and growth epiphysis.
Consequently, it may result in loss of motion, pain, leg-length
discrepancy, consequent limp, and early osteoarthritis.1Y13
Surgical treatment of the sequelae may be indicated to
improve the joint condition and aspect, providing the best
function possible at the adulthood. To guide treatment, some
radiographic classications have been proposed. The most
referred is the Choi et al,14 a modication of the Hunka et al15
system. It classied the hips in 4 types and 8 subtypes, but
the classication is complex and difcult to apply in young
children when treatment may be desirable. We believe that
the 2 most important aspects for treatment and prognosis
are the instability and the grade of the destruction of the
proximal femur.
In this study, we present a series of patients with sequelae of SAH and a simple new classication for sequelae.
We compared it with the classication and results published
by Choi et al.14
METHODS
We retrospectively reviewed the medical records and
radiographs of all patients who had been treated at the Pequeno
Principe Hospital between 1985 and 1997 for SAH. Most
patients in this study were treated at other medical centers at
the acute phase and were referred to our hospital to treat
complications. The diagnosis was made with typical history
of SAH and characteristic signs of the sequelae. Conrmation by culture was not necessary.
The criteria to be included in this study were the
following:
1. children with history of developed septic arthritis before
age of 3 years,
2. minimal age of last clinical and radiographic evaluation
of 4 years or at least 2 years of follow-up for the patients
who underwent reconstruction, and
J Pediatr Orthop
& Volume 28, Number 5, July/August 2008
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
J Pediatr Orthop
& Volume 28, Number 5, July/August 2008
Sequelae of Pediatric Septic Arthritis of the Hip
3. patients seen at our institution without previous treatment
of the sequelae.
We excluded all patients with minimal sequelae (type 1
by Choi et al classication), tuberculosis, and neurological
involvement and the ones whose diagnosis of bacterial
infection was not clear.
Forty-one hips in 37 patients met the criteria to be
included in this study. There were 24 boys and 13 girls. The
right side was involved in 16 patients; the left side, in 17;
and bilateral, in 4. Twenty-ve patients presented the acute
disease when newborn; and 16, between ages of 1 month
and 3 years. Twenty-one patients had late drainage (at least
5 days after onset), and 20 did not undergo drainage.
Fifteen hips underwent a reconstruction procedure: open
reduction (OR) in 6, OR associated with Dega osteotomy in
5, OR associated with Dega and varus proximal femoral
osteotomy in 2, and OR associated with Salter osteotomy in
2 hips.
Seventeen hips were submitted to other modalities of
surgeries: valgus proximal femur osteotomy in 9, shelf
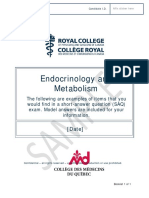
FIGURE 2. Our classication.
procedure in 3, distal transfer of the great trochanter in 3, and
Steel osteotomy in 1 hip. Three of these patients also had an
epiphysiodesis of the contralateral distal femur associated.
Other 9 hips had no surgery.
Radiographic Classication
We classied the hips using 2 different classications:
1. The method proposed by Choi et al14 in their original
article (Fig. 1). There were 18 hips classied as type 2A, 4
as 2B, 1 as 3A, 1 as 3B, 7 as 4A, and 10 as 4B.
2. Our classication (Fig. 2). It was based on the relation
between the femur and the acetabulum (1 or 2) and at the
severity of the lesion of the proximal femur (A or B).
Therefore, the classication has 2 groups and 2 subgroups:
& grade 1, hips with the head or the femoral neck within
the acetabulum. It was subdivided in A when the femoral
head (total or part of) was present and B when it was
absent.
& grade 2, hips are dislocated. It was also subdivided in A
if the femoral head was present and B when it was
absent.
There were 10 hips classied as 1A, 11 as 1B, 3 as 2A,
and 17 as 2B.
Comparing the Two Systems of Classication
FIGURE 1. Classication as published by Choi et al. (From Choi
et al. Sequelae and reconstruction after septic arthritis of the hip
in infants. J Bone Joint Surg [Am]. 1990;72-A:1150Y1164.
To assess the concordance of both classications, 3 independent senior pediatric orthopaedic surgeons evaluated the
initial radiography of each case. They were not aware of the
patient condition, treatment, or outcome. We asked them to
classify the hips using both systems.
The surgeons were given Choi et al14 original drawing
and explanation as published. Our classication consisted of
an explanation through text and illustrations as shown here.
* 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
525
Forlin and Milani
J Pediatr Orthop
& Volume 28, Number 5, July/August 2008
FIGURE 3. A, Radiograph of a patient who presents a septic arthritis of the right hip as a newborn. B, At age of 8 years, there is
some degree of subluxation and dysplasia (type 1A sequelae). C, As the subluxation progresses and the patient presented pain, a
shelf acetabuloplasty was performed at age of 10 years. At the age of 13 years and 5 months, the radiograph shows a good joint
coverage.
No other explanation was provided. The analysis of the 3
surgeons and the authors was used for statistical evaluation.
We also compared our series of patients and results with
those reported by Choi et al.14 To do that, we divided their
patients in 2 groups by the stability criteria. Those classied as
types 1, 2, and 3 were considered stable, and the type 4 was
considered unstable. For our classication, grade 1 was considered stable; and grade 2, unstable.
Study of the Authors Classication
and Variables
Classication of the Results
The average age at the last visit was 9.9 years (range,
3.9Y19 years). The average length of follow-up from the rst
surgery for the treatment of the sequelae was 5.2 years (range, 3
months to 11.3 years). For the patients who underwent reconstruction, the mean follow-up was 6.9 years (range, 2.7Y11.3 years).
Thirty-seven hips were pain-free, and 4 presented
pain. Thirty-seven hips had a satisfactory range of motion
(90.2%). Stability was present in 29 hips (70.7%), and 12 were
unstable (29.3%).
Final results showed 24 hips classied as satisfactory
and 17 as unsatisfactory.
In the group of reconstructed hips, 14 of them were
painless. A satisfactory range of motion was present in 13
hips. Eleven hips were stable, and 4 were unstable. At the end,
8 were classied as satisfactory; and 7, as unsatisfactory.
Of the 26 hips without a reconstruction surgery, 23
were pain-free, and 3 presented pain; 24 had a satisfactory
range of motion, and 2 had not; 18 were stable, and 8 were
Using the classication proposed by the author, we
consider the possibility of a relationship between sequelae
with sex, side, age at time of the acute infection, performance
of drainage or not, reconstruction surgery, and results.
RESULTS
The results were classied clinically by Hunka et al15
criteria. Satisfactory results had the following conditions:
1. the joint was stable,
2. range of motion of 50 degrees or more of exion and a
exion contraction below 20 degrees, and
3. a painless hip for the daily activities.
The hip was classied as unsatisfactory when one or
more criteria above were present.
Statistical Analysis
We considered full concordance when all 4 surgeons
came up with the same grade or type for the analyzed hip.
A W2 test and a Fisher exact test were used for notemporal variable and t-student for temporal.
The decisions for statistic test were based on 5% or
0.05 signicance.
FIGURE 4. A, Radiograph of a 13-year-old boy with a sequelae type 1A at the left side showing a subluxation that was
progressive. B, After a Steel triple osteotomy, there is improvement at the joint relationship, but some incongruence remains.
C, Important narrowing of the joint space was noticed, and a valgus osteotomy was performed. The result was unsatisfactory with
ankylosis of the hip.
526
* 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
J Pediatr Orthop
& Volume 28, Number 5, July/August 2008
Sequelae of Pediatric Septic Arthritis of the Hip
FIGURE 5. A, Radiograph of a patient at age 1 year and 3 months who developed an SAH as a newborn presenting type 2B sequelae
submitted to an OR and a Dega osteotomy. B, At age of 5 years and 2 months, a well-centered hip is seen. It was classied as a
satisfactory result.
unstable. The nal result was satisfactory in 16 hips and unsatisfactory in 10.
Full concordance was found in 25 of 41 hips for the
classication proposed by the authors and in 7 of 41 hips using
the Choi et al system (P = 0.01).
Of the 25 hips in patients who had the acute phase at
neonatal age, 7 had sequelae 1A or 1B, and 18 presented
sequelae 2A or 2B. Of the 16 who had the infection late, only
2 had a grade 2A or 2B sequelae (signicant difference).
Of the 21 classied as sequelae grade 1A or 1B, 16 hips
(77%) presented a satisfactory result. Of the 20 sequelae
grade 2A or 2B, only 8 (40%) presented a satisfactory result
(P = 0.00).
There were no statistical relations between grades of sequelae and the gender, side, and delay for drainage or no drainage.
There were no differences, based on stability criteria
before treatment between the group of patients from our study
and the one published by Choi et al (P = 0.36). Also, there
were no differences in the results for both studies (P = 0.73).
DISCUSSION
The diagnosis of SAH in infants and especially in
newborns may be difcult.6,9,11,14 Many cases have delayed
diagnosis and treatment causing devastating complications
leading to decrease of life quality, multiple medical procedures,
and hospitalizations with a high social and economic cost.
Some factors are related with the occurrence of the
sequelae: age at the time of infection, prematurity, newborns
that needed intensive care, type of bacteria, and delay of the
treatment.1,2,4Y6,8,9,11,13 Most of the authors agree that a delay of
4 days or more increases the chance of bad prognosis.1,5,16,17
Only 21 hips of this series underwent surgical drainage at the
acute phase. All of them had a delay of 5 days or more.
Two anatomical factors may contribute for the poor results in young patients. The presence of intraarticular metaphysis allows dissemination from bone to joint. Also, if the
main blood supply of the femoral head is intraarticular, the
increase of pressure may cause avascular necrosis.18Y21 In our
series, the newborns presented a worse result. Of the 25 hips
that had the acute disease as a newborn, 18 had more severe
sequelae. Because we did not study children without sequelae, we cannot afrm that newborns have worse progno-
sis to develop sequelae; however, if they do, sequelae will be
more severe.
Sequelae may vary from very subtle alteration to severe
destruction of the proximal femur and dislocation of the joint.
It makes important to have a classication useful to treatment
decision and prognosis. We realized that the Choi et al14
classication describes in details the anatomical alterations,
and thus, it became the referred method. However, the number of types and details of each one may make it difcult to
reach an agreement by different observers and do not allow
drawing signicant conclusions.
We agree that the evaluation of an immature hip, mostly
formed by cartilaginous tissue, may not represent the real anatomical situation.9 Uses of arthrography or magnetic resonance
imaging are effective to demonstrate the nonosseous structure.
However, these examinations may not be available, have high
costs, and/or require anesthesia. In addition, we do not have
studies that provide a reliable correlation between their ndings
and the nal outcome. Roentgenograms are still the standard for
the evaluation.
Our proposal of classication intends to be simple, analyzing factors that could be important for the decision of
treatment: instability and the presence of the femoral head. A
study of concordance showed that it has less interobserver
variability than the one proposed by Choi et al14 (full
concordance of 25 in 41 hips against 7 in 41). Only on 5
hips, there was no concordance for the stability criteria (eg, for
the same hip, 2 surgeons classied as grade 1 and 1 classied
in grade 2).
Comparing the patients and results presented by Choi
et al14 and those presented to us, no differences were found.
There were 13 unstable hips (types 4A and 4B) and 21 stable
hips (types 1, 2, and 3) in the Choi et al14 study and 20
unstable and 21 stable hips for our classication (P = 0.37).
The results obtained also did not present signicant differences either for stable (P = 0.73) or unstable hips (P = 0.72).
For these reasons, it seems more appropriate to use the simplest classication.
Hips with type 1 sequelae had a much better prognosis, and the treatment goal was diverse. The procedures in
these hips are indicated to correct acetabular dysplasia or to
improve congruence. For this, we prefer the shelf procedure
or a proximal femoral valgus osteotomy. Both are safe and
* 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
527
J Pediatr Orthop
Forlin and Milani
can be done with an irregular femoral head (Figs. 3AYC). The
redirectional osteotomies like Salter or Steel may increase
the pressure leading do stiffness (Figs. 4AYC).
Treatment of type 2 sequelae is controversial. Some
authors (Betz et al3 and Wopperer et al22) do not recommend
treatment because of the good functional results in patients
who did not undergo reconstruction. They only recommended contralateral epiphysiodesis to address the leg-length
discrepancy. Many others recommended reconstruction, but
there is no consensus about the procedure to be used.14,23Y31
Because of the risk of the stiffness, a proximal femoral valgus
osteotomy concomitant with lengthening of distal femur and
external xation was proposed.31,32
Like many authors, we prefer to perform the reconstruction in a young child.9,14,15,22 Better results were obtained
with the association of concomitant OR, proximal femoral
varus osteotomy, and Dega acetabuloplasty (Figs. 5A, B).
Although treatment can transform the unstable hip (type 2)
in a stable one (type 1), theoretically improving the prognosis,
we are aware that the results may be deteriorated after a
longer follow-up.
Leg-length discrepancy should be expected in all patients with lesion of the proximal epiphysis. In the stable hips,
the discrepancy varies from 2 to 5 cm, and for the unstable
hips, it reaches up to 14 cm. In our series, the maximum discrepancy in the centered hip (with or without reconstruction)
was 4.5 cm at the last follow-up. Epiphysiodesis of the contralateral distal femur would be the choice for these patients.
In a comparable group of patients, our classication
showed to be simpler and more reliable than those published
by Choi et al14 and may be useful for the prognosis and as
an indicator of treatment. Controversy still remains if the unstable hips will benet from the reconstruction procedures.
REFERENCES
1. Bennett OM, Namnyak SS. Acute septic arthritis of the hip joint in
infancy and childhood. Clin Orthop. 1992;281:123Y132.
2. Berdahl S, Ekengren K, Eriksson M. Neonatal hematogenous osteomyelitis: risk factors for long-term sequelae. J Pediatr Orthop.
1985;5:564Y568.
3. Betz RR, Cooperman DR, Wopperer JM, et al. Late sequelae of septic
arthritis of the hip in infancy and childhood. J Pediatr Orthop.
1990;10:365Y372.
4. Chacha PB. Suppurative arthritis of the hip joint in infancy: a persistent
diagnostic problem and possible complication of femoral venipuncture.
Bone Joint Surg Am. 1971;53-A(3):538Y544.
5. Fabry G, Meire E. Septic orthritis of the hip in children: poor
results after late and inadequate treatment. J Pediatr Orthop.
1983;3:461Y466.
6. Gillespie R. Septic arthritis of childhood. Clin Orthop. 1973;96:
152Y159.
7. Grill F, Rustler T. Late sequelae of coxitis in infants. Orthopade.
1997;26(10):848Y857.
8. Howard JB, Highgenboten CL, Nelson JD. Residual effects of septic
arthritis in infancy and childhood. JAMA. 1976;236(8):932Y935.
528
& Volume 28, Number 5, July/August 2008
9. Mitchell GP. Management of acquired dislocation of the hip in septic
arthritis. Orthop Clin North Am. 1980;11:51Y64.
10. Morrey BF, Bianco AJ, Rhodes KH. Suppurative arthritis of the hip in
children. J Bone Joint Surg Am. 1976;58-A(3):388Y392.
11. Morrissy RT. Bone and joint infection in the neonate. Pediatr Ann.
1989;18:36Y44.
12. Obletz BE. Acute suppurative arthritis of the hip in the neonatal period.
J Bone Joint Surg Am. 1960;42-A(1):23Y30.
13. Peters W, Irving J, Letts M. Long-term effects of neonatal bone and joint
infection on adjacent growth plates. J Pediatr Orthop. 1992;
12:806Y810.
14. Choi IH, Pizzutillo PD, Bowen JR, et al. Sequelae and reconstruction after
septic arthritis of the hip in infants. J Bone Joint Surg Am. 1990;72:
1150Y1165.
15. Hunka L, Said SE, MacKenzie DA, et al. Classification and surgical
management of the severe sequelae of septic hips in children. Clin Orthop.
1982;171:30Y36.
16. Lunseth PA, Heiple KG. Prognosis in septic arthritis of the hip in children.
Clin Orthop. 1979;139:81Y85.
17. Parsch K, Savvidis E. Coxitis in the newborn and infant: diagnosis and
therapy. Orthopaedic. 1997;26(10):838Y847.
18. Chung SMK. The arterial supply of the developing proximal end of the
human femur. J Bone Joint Surg Am. 1976;58-A(7):961Y970.
19. Kemp HBS, Lloyd-Roberts GC. Avascular necrosis of the capital
epiphysis following osteomyelitis of the proximal femoral metaphysis.
J Bone Joint Surg Br. 1974;56-B(4):688Y697.
20. Trueta J. The normal vascular anatomy of the human femoral head during
growth. J Bone Joint Surg Br. 1957;39-B(2):358Y394.
21. Vidigal EC Jr, Vidigal EC, Fernandes JL. Avascular necrosis as a
complication of septic arthritis of the hip in children. Int Orthop.
1997;1(6):389Y392.
22. Wopperer JM, White JJ, Gillespie R, et al. Long-term follow-up of
infantile hip sepsis. J Pediatr Orthop. 1988;8:322Y325.
23. Forlin E, Cunha LAM, Kamp PA, et al. Tratamento das sequelas da artrite
septica do quadril na crian0a. Rev Bras Ortop. 1992;27:299Y305.
24. Freeland AE, Sullivan DJ, Westin GW. Greater trochanteric hip
arthroplasty in children with loss of the femoral head. J Bone Joint Surg
Am. 1980;62:1351Y1361.
25. Hallel T, Salvati EA. Septic arthritis of the hip in infancy: end result study.
Clin Orthop. 1978;132:115Y128.
26. Harmon PH. Surgical treatment of the residual deformity from
suppurative arthritis of the hip occurring in young children. J Bone Joint
Surg Am. 1942;24:576Y585.
27. Wang EB, Ji SJ, Zhao Q, et al. Treatment of severe sequelae of infantile
hip sepsis with trochanteric arthroplasty. J Pediatr Orthop.
2007;2:165Y170.
28. Rigault P, Lagrange J, Pouliquen JC, et al. La trochanteroplastie.
Operation de sauvetage dans les mutilations de la tete et du col du femur
chez lenfant. Indications, technique et resultats a` propos de 10 cas. Revue
Chir Orthop. 1973;59:565Y582.
29. Weissman SL. Transplantation of the trochanteric epiphysis into the
acetabulum after septic arthritis of the hip. Report of a case. J Bone Joint
Surg Am. 1967;49:1647Y1651.
30. Krumins M, Kalnins J, Lacis G. Reconstruction of the proximal end of
the femur after hematogenous osteomyelitis. J Pediatr Orthop. 1993;
13:63Y67.
31. Cheng JC, Aguilar J, Leung PC. Hip reconstruction for femoral head loss
from septic arthritis in children: a preliminary report. Clin Orthop.
1995;314:214Y224.
32. Cheng JCY, Lam TP. Femoral lengthening after type IVB septic arthritis
of the hip in children. J Pediatr Orthop. 1996;16:533Y539.
33. Choi IH, Shin YW, Chung CY, et al. Surgical treatment of the severe
sequelae of infantile septic arthritis of the hip. Clin Orthop.
2005;434:102Y109.
* 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Nursing Care (Bing 1)Dokument6 SeitenNursing Care (Bing 1)Shafira ChusnaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Gigantism (Final)Dokument10 SeitenGigantism (Final)Bonifacio SandongNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Edit - HIL - Daily IGD 25.09.19Dokument30 SeitenEdit - HIL - Daily IGD 25.09.19Inez WijayaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- VR HSGDokument12 SeitenVR HSGNirupa RamachandranNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Tubal LigationDokument3 SeitenTubal LigationPal_inNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- PolypsDokument2 SeitenPolypsjsdlzjNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Choosing Between Colloids and Crystalloids For IV InfusionDokument4 SeitenChoosing Between Colloids and Crystalloids For IV InfusionFamily Prepper100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Presentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONDokument23 SeitenPresentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONMubarak M AlkaliNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- StaffingDokument33 SeitenStaffingshalini75Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- ThyroidDokument16 SeitenThyroidnawaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Promotion 2013-2014 With AnswerDokument36 SeitenPromotion 2013-2014 With AnswerAloah122346Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Worksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Dokument3 SeitenWorksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Emerald SpanglerNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Module 5 Activity 1Dokument1 SeiteModule 5 Activity 1Hannah CaseriaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Endocrinology Metabolism Saq Sample Exam eDokument11 SeitenEndocrinology Metabolism Saq Sample Exam eعمر كمالNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Gynius Brochure 2020Dokument8 SeitenGynius Brochure 2020BINIYAM TADESSENoch keine Bewertungen
- Elderly IncontinenceDokument4 SeitenElderly IncontinenceJonas Marvin AnaqueNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Standard Bill FormatDokument14 SeitenStandard Bill FormatPrasanna Nammalwar100% (1)
- Bsc. Nursing Examination: Revision QuestionsDokument79 SeitenBsc. Nursing Examination: Revision QuestionsNixi MbuthiaNoch keine Bewertungen
- Wrist PainDokument8 SeitenWrist PainLev KalikaNoch keine Bewertungen
- Form 3341Dokument2 SeitenForm 3341Harish ChandNoch keine Bewertungen
- Birdem Day Visit-K65 (Masud)Dokument10 SeitenBirdem Day Visit-K65 (Masud)Anonymous XqNRxzm1xNoch keine Bewertungen
- Mother & Child Hospital Planning & Designing: Info@hhbc - inDokument8 SeitenMother & Child Hospital Planning & Designing: Info@hhbc - inwrightwoman100% (1)
- Care 2000Dokument9 SeitenCare 2000Sneha_Sawant_4900100% (2)
- ANTENATAL CARE Translate GooglingDokument26 SeitenANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- DEA InformationDokument12 SeitenDEA Informationkdavis618Noch keine Bewertungen
- SpesMedica 10 Catalogo de NeurologiaDokument50 SeitenSpesMedica 10 Catalogo de NeurologiaIsmael Isaac Rios Jose0% (1)
- Avalon - FM20 - and - FM30 Bro New PDFDokument4 SeitenAvalon - FM20 - and - FM30 Bro New PDFNugie DamayantoNoch keine Bewertungen
- Neonatal Resuscitation Algorithm For ZambiaDokument2 SeitenNeonatal Resuscitation Algorithm For ZambiaBassim Birkland100% (2)
- Case StudyDokument30 SeitenCase StudyPeter Crabajales50% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Prevention of Surgical Site Infections: Pola Brenner, Patricio NercellesDokument10 SeitenPrevention of Surgical Site Infections: Pola Brenner, Patricio NercellesAmeng GosimNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)