Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Brij Pal Vs StateDokument7 SeitenBrij Pal Vs StateSatyendra ChauhanNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Running Head: Ethical Policy-Making ExerciseDokument12 SeitenRunning Head: Ethical Policy-Making Exerciseapi-160674927Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Quality CircleDokument40 SeitenQuality CircleMuhammad KashifNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Dwnload Full Criminal Behavior A Psychological Approach 10th Edition Bartol Test Bank PDFDokument35 SeitenDwnload Full Criminal Behavior A Psychological Approach 10th Edition Bartol Test Bank PDFgrobesonnie100% (15)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Regulatory Framework AND Legal Issues IN Business: Cristine G. Policarpio Bsais 3-BDokument33 SeitenRegulatory Framework AND Legal Issues IN Business: Cristine G. Policarpio Bsais 3-BApril Joy SevillaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Vwca AgreementDokument51 SeitenVwca Agreementworkcovervictim8242Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Political Order in Changing SocietiesDokument83 SeitenPolitical Order in Changing SocietiesMichiru2011100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Why Should I Be Moral?Dokument1 SeiteWhy Should I Be Moral?Bang BangNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- B325 MTA 2017-2018- ساره هلال الخالدي- second courseDokument14 SeitenB325 MTA 2017-2018- ساره هلال الخالدي- second courseAmethyst Online67% (3)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Work ImmersionDokument11 SeitenWork ImmersionSherwin Jay BentazarNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- 1 Estate of Hemady v. Luzon SuretyDokument2 Seiten1 Estate of Hemady v. Luzon SuretyTherese EspinosaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- MBTI Personality Type Test: Name: - Roll NoDokument4 SeitenMBTI Personality Type Test: Name: - Roll NoSaurabh Kulkarni 23100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- (Labor 2 - Atty. Nolasco) : G.R. No. 196539 Perez, J. Digest By: IntiaDokument2 Seiten(Labor 2 - Atty. Nolasco) : G.R. No. 196539 Perez, J. Digest By: IntiaRaymund CallejaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Position PaperDokument9 SeitenPosition PaperJamellen De Leon BenguetNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Business Ethics: Felix M. Del Rosario, Cpa, MbaDokument38 SeitenBusiness Ethics: Felix M. Del Rosario, Cpa, Mbafelix madayag del rosarioNoch keine Bewertungen
- G..26160B.tension Carriage.508.512Dokument3 SeitenG..26160B.tension Carriage.508.512Jean ChungNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- NSTP (LTS) Activity 1 Ma. Nicole Pateño: 1. Give Your Own Perspective About The VMGO of BISU?Dokument3 SeitenNSTP (LTS) Activity 1 Ma. Nicole Pateño: 1. Give Your Own Perspective About The VMGO of BISU?MA. NICOLE PATENONoch keine Bewertungen
- Kim Basinger Vs MLP Oral AgreementDokument31 SeitenKim Basinger Vs MLP Oral AgreementrafiqNoch keine Bewertungen
- Academic Honesty Statement: Writing at Carson-Newman CollegeDokument1 SeiteAcademic Honesty Statement: Writing at Carson-Newman CollegeGlenn TaduranNoch keine Bewertungen
- CALIFORNIA MASONIC CODE - Masons of California PDFDokument287 SeitenCALIFORNIA MASONIC CODE - Masons of California PDFJose F Vela Rondon100% (1)
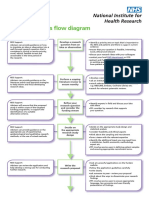
- Research Process Flow Chart A4 WebDokument2 SeitenResearch Process Flow Chart A4 WebEma FatimahNoch keine Bewertungen
- Melody Gardot Your Heart Is As Black As NightDokument8 SeitenMelody Gardot Your Heart Is As Black As NightmiruNoch keine Bewertungen
- Rose DoneganDokument2 SeitenRose DoneganAnish GeorgeNoch keine Bewertungen
- Character and Symbol in Shakespeare 039 S Plays A Study of Certain Christian and Pre Christian Elements in Their Structure and Imagery Cambridge LiDokument224 SeitenCharacter and Symbol in Shakespeare 039 S Plays A Study of Certain Christian and Pre Christian Elements in Their Structure and Imagery Cambridge Limicuta87100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Araneta Vs GatmaitanDokument1 SeiteAraneta Vs GatmaitanXyra Krezel GajeteNoch keine Bewertungen
- Maintenance and Welfare of Parents and Senior Citizens ActDokument12 SeitenMaintenance and Welfare of Parents and Senior Citizens ActKrishna PrasadNoch keine Bewertungen
- G.R. No. 154410 HeavyliftDokument20 SeitenG.R. No. 154410 HeavyliftKenshin HealerNoch keine Bewertungen
- Building Partnership and Linkages: Youth Formation DivisionDokument35 SeitenBuilding Partnership and Linkages: Youth Formation DivisionLeven Mart LacunaNoch keine Bewertungen
- Attached: DR Amir Levine and Rachel HellerDokument18 SeitenAttached: DR Amir Levine and Rachel HellersupercellxmikuNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Legal Rights and DutiesDokument7 SeitenLegal Rights and DutiesHutiya KumNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)