Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- VascularDisordersLiver2009 PDFDokument36 SeitenVascularDisordersLiver2009 PDFmalik003Noch keine Bewertungen
- SummariesDokument140 SeitenSummariesmalik003Noch keine Bewertungen
- Visa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSDokument1 SeiteVisa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSmalik003Noch keine Bewertungen
- Recent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A ReviewDokument18 SeitenRecent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A Reviewmalik003Noch keine Bewertungen
- Career Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017Dokument2 SeitenCareer Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017malik003Noch keine Bewertungen
- Bleeding Disorder ApproachDokument9 SeitenBleeding Disorder Approachmalik003Noch keine Bewertungen
- Recommendations For Testing, Managing, and Treating Hepatitis C - HCV TESTING and LINKAGE To CARE - 2015-06-29Dokument12 SeitenRecommendations For Testing, Managing, and Treating Hepatitis C - HCV TESTING and LINKAGE To CARE - 2015-06-29malik003Noch keine Bewertungen
- April 24: Zein Mahgoub PACES Simplified Zein MahgoubDokument4 SeitenApril 24: Zein Mahgoub PACES Simplified Zein Mahgoubmalik003Noch keine Bewertungen
- Dha Exam..Muhammad IbrahimDokument11 SeitenDha Exam..Muhammad Ibrahimmalik003100% (4)
- Recommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29Dokument8 SeitenRecommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29malik003Noch keine Bewertungen
- 5446.full 2Dokument12 Seiten5446.full 2malik003Noch keine Bewertungen
- History in Ob/Gy: Ahmed AbdulwahabDokument9 SeitenHistory in Ob/Gy: Ahmed Abdulwahabmalik003Noch keine Bewertungen
- Cranial Nerve AssessmentDokument42 SeitenCranial Nerve Assessmentmalik003100% (1)
- Urgent Required Female Staff NursesDokument1 SeiteUrgent Required Female Staff Nursesmalik003Noch keine Bewertungen
- Unilateral Enlarged Kidney PDFDokument2 SeitenUnilateral Enlarged Kidney PDFmalik003Noch keine Bewertungen
- 6868841Dokument35 Seiten6868841malik003Noch keine Bewertungen
- Prevention of Venous Thromboembolism in Nonsurgical PatientsDokument23 SeitenPrevention of Venous Thromboembolism in Nonsurgical Patientsmalik003Noch keine Bewertungen
- CVS PDFDokument102 SeitenCVS PDFmalik003Noch keine Bewertungen
- GR 080013Dokument3 SeitenGR 080013malik003Noch keine Bewertungen
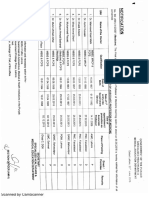
- Associate Med PDFDokument2 SeitenAssociate Med PDFmalik003Noch keine Bewertungen
- New Doc 44 - 1Dokument1 SeiteNew Doc 44 - 1malik003Noch keine Bewertungen
- 1000 Prometric MCQ Solved 2Dokument351 Seiten1000 Prometric MCQ Solved 2chronos653490% (106)
- Associate MedDokument2 SeitenAssociate Medmalik003Noch keine Bewertungen
- Assoc Prof MedDokument1 SeiteAssoc Prof Medmalik003Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Requirements Specification For Patient Level Information and Costing Systems (PLICS) Mandatory Collections Continued ImplementationDokument40 SeitenRequirements Specification For Patient Level Information and Costing Systems (PLICS) Mandatory Collections Continued ImplementationAbidi HichemNoch keine Bewertungen
- PRN00284 Health Building Note 16 01 Facilities For Mortuaries Including Body Stores and Post Mortem ServicesDokument114 SeitenPRN00284 Health Building Note 16 01 Facilities For Mortuaries Including Body Stores and Post Mortem ServicesmohamedmizoNoch keine Bewertungen
- Case Study ST HelensDokument2 SeitenCase Study ST HelensQuoc Ty TranNoch keine Bewertungen
- Consultant Ophthalmologist - GlaucomaDokument23 SeitenConsultant Ophthalmologist - GlaucomaAli HassanNoch keine Bewertungen
- 7424 Personal SpaceDokument28 Seiten7424 Personal SpaceJoyce Ellen Hernandez JavierNoch keine Bewertungen
- HTM 05-03 Part F FinalDokument20 SeitenHTM 05-03 Part F FinalRashidNoch keine Bewertungen
- Neethu Mohan - Hillingdon Hospital NHS Foundation Trust - Conditional Offer LetterDokument4 SeitenNeethu Mohan - Hillingdon Hospital NHS Foundation Trust - Conditional Offer LetterKevin George ArackalNoch keine Bewertungen
- Nhs Job Reference TemplateDokument5 SeitenNhs Job Reference Templatee771k2gb100% (1)
- Case Study 3Dokument11 SeitenCase Study 3sheilaNoch keine Bewertungen
- Nimhe 10 High Impact ChangesDokument57 SeitenNimhe 10 High Impact ChangesMatías ArgüelloNoch keine Bewertungen
- Improving Patient Safety PDFDokument183 SeitenImproving Patient Safety PDFwawanNoch keine Bewertungen
- Pharma Company Organizational StructureDokument72 SeitenPharma Company Organizational StructureDhiraj Shukla100% (5)
- SNP Yes LeafletDokument8 SeitenSNP Yes LeafletThe SpectatorNoch keine Bewertungen
- Financial Modelling CVDokument3 SeitenFinancial Modelling CVGanapathiraju SravaniNoch keine Bewertungen
- Blood Transfusion Single Use PathwayDokument6 SeitenBlood Transfusion Single Use PathwayropusanNoch keine Bewertungen
- RCSLT BulletinDokument32 SeitenRCSLT Bulletinlionella12Noch keine Bewertungen
- Care Homes: Finding, Choosing and Paying For A Care HomeDokument44 SeitenCare Homes: Finding, Choosing and Paying For A Care HomeNasroNoch keine Bewertungen
- GWS Total Hip ReplacementDokument17 SeitenGWS Total Hip ReplacementRadu MoglanNoch keine Bewertungen
- Rehabilitation Rcpsych Report 2009Dokument46 SeitenRehabilitation Rcpsych Report 2009psychforall100% (2)
- Public Health Policy: January 2003Dokument17 SeitenPublic Health Policy: January 2003Febiyanti Afitia100% (1)
- Demographics and Leadership Philosophy: Exploring Gender DifferencesDokument33 SeitenDemographics and Leadership Philosophy: Exploring Gender DifferencesDaniela Maria Barrientos GuzmanNoch keine Bewertungen
- UK Immigration Consultants General InformationDokument4 SeitenUK Immigration Consultants General Informationexpert0% (1)
- Laundry ProcedureDokument6 SeitenLaundry ProcedureSenthil Kumar0% (1)
- Step by Step Process of Becoming A United Kingdom Registered NurseDokument3 SeitenStep by Step Process of Becoming A United Kingdom Registered NurseKoffi Agbéko HonsouNoch keine Bewertungen
- Wilson, Dillon - EPQ Essay Final (Dec 2014)Dokument18 SeitenWilson, Dillon - EPQ Essay Final (Dec 2014)Dillon WilsonNoch keine Bewertungen
- DH 4012286Dokument5 SeitenDH 4012286Edwin KurniawanNoch keine Bewertungen
- The Community Voice For Wanstead, Snaresbrook and AldersbrookDokument6 SeitenThe Community Voice For Wanstead, Snaresbrook and AldersbrookWoodhorneNoch keine Bewertungen
- GPC 466 Ictus AP Lain Entr Compl enDokument230 SeitenGPC 466 Ictus AP Lain Entr Compl enLucas AresNoch keine Bewertungen
- Community Mental Health Framework For Adults and Older AdultsDokument22 SeitenCommunity Mental Health Framework For Adults and Older AdultsLuigi LuiNoch keine Bewertungen
- "This Is How It Feels To Be Lonely" - A Report On Migrants and Refugees' Experiences With Loneliness in LondonDokument28 Seiten"This Is How It Feels To Be Lonely" - A Report On Migrants and Refugees' Experiences With Loneliness in LondonMigrants OrganiseNoch keine Bewertungen