Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Biomechanicks of Snatch Technique of Hghly Skilled and Skilled WeigthliftersDokument6 SeitenBiomechanicks of Snatch Technique of Hghly Skilled and Skilled WeigthliftersStuarNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Prosthetic Foot Project PDFDokument45 SeitenProsthetic Foot Project PDFtesterNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Range of MotionDokument59 SeitenRange of MotionIsrael Jiel Fedelicio100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Angles90 Instructions ENDokument7 SeitenAngles90 Instructions ENStéphaneNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- 5 DNSA Treatment PDFDokument9 Seiten5 DNSA Treatment PDFklinik bapelkes ksNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Positioning PadDokument36 SeitenPositioning PadLeonila RoyoNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Rotator Cuff InjuriesDokument26 SeitenRotator Cuff Injuriesanname_girlNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Chair Yoga HandoutDokument2 SeitenChair Yoga HandoutRachel Mecali100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Anatomy, Pathophysiology, Andbiomechanics of Shoulder InstabilityDokument9 SeitenAnatomy, Pathophysiology, Andbiomechanics of Shoulder InstabilityDelaram IravaniNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A. Ectoderm. B. Mesoderm (Correct Answer) C. Endoderm D. All of The AboveDokument94 SeitenA. Ectoderm. B. Mesoderm (Correct Answer) C. Endoderm D. All of The AboveMojahed Al Jaafri100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Neurological Examination in Psychiatry: Abid Rizvi Junior Resident 3 Department of PsychiatryDokument149 SeitenNeurological Examination in Psychiatry: Abid Rizvi Junior Resident 3 Department of PsychiatryMohammed ArarNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Infant BehaviorDokument14 SeitenInfant BehaviorNiña RevesencioNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
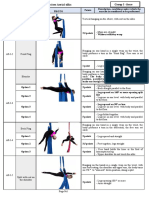
- Appendix 1 Compulsory Exercises Aerial Silk Eng 2018Dokument23 SeitenAppendix 1 Compulsory Exercises Aerial Silk Eng 2018tito1628100% (6)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Neill - A To Z of Bones JT & LigamentDokument272 SeitenNeill - A To Z of Bones JT & LigamentPaul Vk100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Joe Muscolino - 7 Keys To Neck Posture 2-10Dokument5 SeitenJoe Muscolino - 7 Keys To Neck Posture 2-10frsh100% (1)
- 87 Slides Fundamentals in Orthopedic Surgery 2019Dokument88 Seiten87 Slides Fundamentals in Orthopedic Surgery 2019Mark Samuel Tanchoco100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Principles of Tendon TransfersDokument17 SeitenPrinciples of Tendon TransfersGirijashankar KhuntiaNoch keine Bewertungen
- Synopsis Template - MPTR 2022 - For Merge-1Dokument13 SeitenSynopsis Template - MPTR 2022 - For Merge-1sriram gopalNoch keine Bewertungen
- Manejo Via Aérea Trauma CervicalDokument26 SeitenManejo Via Aérea Trauma CervicalOdlanier Erwin Castro OlivaresNoch keine Bewertungen
- Glasgocoma ScaleDokument35 SeitenGlasgocoma Scalepop lopNoch keine Bewertungen
- 3 HyperkyphosisDokument11 Seiten3 HyperkyphosisMohammad FoudaNoch keine Bewertungen
- Hip Flexion Strengthening: Therapeutic Exercise For The HipDokument3 SeitenHip Flexion Strengthening: Therapeutic Exercise For The Hipapi-285724474Noch keine Bewertungen
- Trigger Points Quick Reference Student ResourceDokument129 SeitenTrigger Points Quick Reference Student ResourceViviana Rolón100% (2)
- Imci Case StudyDokument47 SeitenImci Case StudyAl-nazer Azer AlNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Open Sim Tutorial 1Dokument10 SeitenOpen Sim Tutorial 1Rayanne FlorianoNoch keine Bewertungen
- Demo Teaching Physical Health AssessmentDokument5 SeitenDemo Teaching Physical Health AssessmentJulie May SuganobNoch keine Bewertungen
- Origin and Historical Foundation of Physical Education and SportsDokument9 SeitenOrigin and Historical Foundation of Physical Education and SportshistoryadorNoch keine Bewertungen
- CP QuadriplegaDokument2 SeitenCP QuadriplegaNamrah AfzalNoch keine Bewertungen
- Knot Tying Manual - EthiconDokument44 SeitenKnot Tying Manual - EthiconAdi Martin100% (4)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Al Kavadlo, Danny Kavadlo - Get Strong - The Ultimate 16-Week Transformation Program For Gaining Muscle and Strength - Using The Power of Progressive Calisthenics-Dragon Door Publications (2017) PDFDokument294 SeitenAl Kavadlo, Danny Kavadlo - Get Strong - The Ultimate 16-Week Transformation Program For Gaining Muscle and Strength - Using The Power of Progressive Calisthenics-Dragon Door Publications (2017) PDFVaibhav SharmaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)