Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Full Sample Science Lb1Dokument161 SeitenFull Sample Science Lb1DariaSivtsova100% (5)
- Assignment: Unit 1 Lesson 1 Important PointsDokument3 SeitenAssignment: Unit 1 Lesson 1 Important PointsHin Wa Leung100% (1)
- The Age of EnlightenmentDokument3 SeitenThe Age of EnlightenmentIoana Botar100% (3)
- Aa GTG 000024Dokument35 SeitenAa GTG 000024Edith Moreno UrzuaNoch keine Bewertungen
- Differential Diagnosis Shoulder ConditionsDokument2 SeitenDifferential Diagnosis Shoulder ConditionsRameshKulkarniNoch keine Bewertungen
- Colon Cancer Screening RecommendationDokument1 SeiteColon Cancer Screening RecommendationkapwattNoch keine Bewertungen
- MHA 2011 Incentive SurveyDokument28 SeitenMHA 2011 Incentive SurveykapwattNoch keine Bewertungen
- Sodium and MyelinolysisDokument2 SeitenSodium and MyelinolysiskapwattNoch keine Bewertungen
- Musculo-Skeletal System: (Trunk, Limbs, and Head)Dokument52 SeitenMusculo-Skeletal System: (Trunk, Limbs, and Head)kapwattNoch keine Bewertungen
- Fault Seal Analysis, UK Noerthern Sea, The Alwyn North Statgjord ExampleDokument5 SeitenFault Seal Analysis, UK Noerthern Sea, The Alwyn North Statgjord ExampleAiwarikiaarNoch keine Bewertungen
- Social SupportDokument8 SeitenSocial SupportRaluka ElenaNoch keine Bewertungen
- Certified in Production and Inventory Management (CPIM)Dokument8 SeitenCertified in Production and Inventory Management (CPIM)dathient76Noch keine Bewertungen
- Exalted: The LunarsDokument41 SeitenExalted: The LunarsSreenivasulu Bathala0% (1)
- Starbucks and Free TradeDokument9 SeitenStarbucks and Free TradeSandraPauwelsNoch keine Bewertungen
- Sample of Interview Protocol - Questions Adopted From Timmons 1994Dokument2 SeitenSample of Interview Protocol - Questions Adopted From Timmons 1994Ash RafNoch keine Bewertungen
- Communication Skills For Pharmacists UkratkoDokument2 SeitenCommunication Skills For Pharmacists UkratkoГоран МарковиќNoch keine Bewertungen
- Beekman - Tomorrow's Technology and You 9eDokument89 SeitenBeekman - Tomorrow's Technology and You 9eJimmy DrakeNoch keine Bewertungen
- Group 4 - Reference and SenseDokument24 SeitenGroup 4 - Reference and SenseMachsunaNoch keine Bewertungen
- Java Programming 9Th Edition Farrell Solutions Manual Full Chapter PDFDokument32 SeitenJava Programming 9Th Edition Farrell Solutions Manual Full Chapter PDFaletheasophroniahae100% (9)
- MedigpsDokument8 SeitenMedigpsAlex HillNoch keine Bewertungen
- Facility Planning - Layout Process 4Dokument102 SeitenFacility Planning - Layout Process 4nouman khan100% (1)
- Geotechnical Engineering - I: B.E. (Civil Engineering) Fourth Semester (C.B.S.)Dokument2 SeitenGeotechnical Engineering - I: B.E. (Civil Engineering) Fourth Semester (C.B.S.)Praveen KumarNoch keine Bewertungen
- Renalyn N. Selloga Housekeeping NC IiDokument9 SeitenRenalyn N. Selloga Housekeeping NC IiAlex GinNoch keine Bewertungen
- Blake and MuttonDokument4 SeitenBlake and Muttonmohitegaurv870% (1)
- Radio - Micro - Bit RuntimeDokument16 SeitenRadio - Micro - Bit RuntimeJohn WestNoch keine Bewertungen
- DOA 19 Leaflet Framini 2p en-GB-ID High-ResDokument2 SeitenDOA 19 Leaflet Framini 2p en-GB-ID High-ResHeri SiswantoNoch keine Bewertungen
- Olympic Message SystemDokument16 SeitenOlympic Message Systemtrevor randyNoch keine Bewertungen
- Action Research 2019Dokument26 SeitenAction Research 2019Gerlynne SegadorNoch keine Bewertungen
- BehaviourDokument16 SeitenBehaviourIshita JainNoch keine Bewertungen
- Jchps 6 (4) 15 Page 286-292 MsreddyDokument7 SeitenJchps 6 (4) 15 Page 286-292 MsreddydwahyusafriNoch keine Bewertungen
- Morane 4 PFN FffsDokument20 SeitenMorane 4 PFN FffsFatmen FataNoch keine Bewertungen
- A Review of Shankuka's TheoryDokument14 SeitenA Review of Shankuka's TheoryrajashreeNoch keine Bewertungen
- Transverse ShearDokument4 SeitenTransverse ShearrajdrklNoch keine Bewertungen
- Maximum Remaining - CodeChefDokument3 SeitenMaximum Remaining - CodeChefShubhi SinghNoch keine Bewertungen
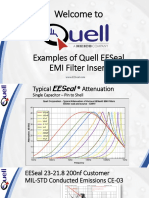
- Examples of Quell's EESeal EMI Filter Inserts - MIL-STD-461 Test ResultsDokument15 SeitenExamples of Quell's EESeal EMI Filter Inserts - MIL-STD-461 Test ResultsXto PeregrinNoch keine Bewertungen