Das könnte Ihnen auch gefallen
- Self-Myofascial Release, Purpose, Methods and TechniquesDokument47 SeitenSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Altered Breathing Patterns During Lumbopelvic Motor ControlDokument8 SeitenAltered Breathing Patterns During Lumbopelvic Motor Controlubiktrash1492Noch keine Bewertungen
- Scapular Positioning and Motor Control in Children and Adults A Laboratory StudyDokument6 SeitenScapular Positioning and Motor Control in Children and Adults A Laboratory StudyCmmb FisioterapiaNoch keine Bewertungen
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDokument10 SeitenScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaNoch keine Bewertungen
- Motion Analysis Study of A Scapular Orientation ExerciseDokument6 SeitenMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaNoch keine Bewertungen
- Self-Myofascial Release, Purpose, Methods and TechniquesDokument47 SeitenSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Review Scapular Positioning and Movement in Unimpaired ShouldersDokument7 SeitenReview Scapular Positioning and Movement in Unimpaired ShouldersCmmb FisioterapiaNoch keine Bewertungen
- Self-Myofascial Release, Purpose, Methods and TechniquesDokument47 SeitenSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Motion Analysis Study of A Scapular Orientation ExerciseDokument6 SeitenMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaNoch keine Bewertungen
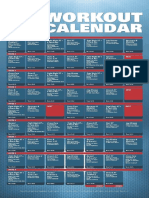
- XT2 Workout Calendar PDFDokument1 SeiteXT2 Workout Calendar PDFYazmin SotoNoch keine Bewertungen
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDokument10 SeitenScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaNoch keine Bewertungen
- Altered Breathing Patterns During Lumbopelvic Motor ControlDokument8 SeitenAltered Breathing Patterns During Lumbopelvic Motor Controlubiktrash1492Noch keine Bewertungen
- Hurdles Performance Lead Arm Technique Advancement For Hurdle PerformanceDokument5 SeitenHurdles Performance Lead Arm Technique Advancement For Hurdle PerformanceCmmb FisioterapiaNoch keine Bewertungen
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDokument10 SeitenScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Neurolymphatic Points Chapmans ReflexesDokument15 SeitenNeurolymphatic Points Chapmans Reflexestaichi7100% (14)
- Procedure Checklist Chapter 37: Teaching A Patient To Cough, Deep-Breathe, Move in Bed, and Perform Leg ExercisesDokument2 SeitenProcedure Checklist Chapter 37: Teaching A Patient To Cough, Deep-Breathe, Move in Bed, and Perform Leg ExercisesjthsNoch keine Bewertungen
- Traditional Dances and Their Characteristic Injury Profiles. Systematic ReviewDokument10 SeitenTraditional Dances and Their Characteristic Injury Profiles. Systematic ReviewSANDRO CASTILLONoch keine Bewertungen
- Hollowing Vs Bracing PDFDokument9 SeitenHollowing Vs Bracing PDFByron Vergara PereiraNoch keine Bewertungen
- Head To Toe AssessmentDokument3 SeitenHead To Toe AssessmentKimberly Witt WhitlockNoch keine Bewertungen
- Lazy Girl WorkoutDokument17 SeitenLazy Girl Workoutسميره محمدNoch keine Bewertungen
- 3 - Summary & MCQs PDFDokument6 Seiten3 - Summary & MCQs PDFSrinivas PingaliNoch keine Bewertungen
- Wolf Motor Function Test WMFTDokument1 SeiteWolf Motor Function Test WMFTTadeja Hernja Rumpf100% (1)
- Bio 2100 Lab 3Dokument19 SeitenBio 2100 Lab 3Kayseri PersaudNoch keine Bewertungen
- A Phlebotomist Extracts What From The Human BodyDokument1 SeiteA Phlebotomist Extracts What From The Human BodyMcj TeeNoch keine Bewertungen
- Introduction To Anatomy:: The Skeletal SystemDokument22 SeitenIntroduction To Anatomy:: The Skeletal SystemShewandagn KebedeNoch keine Bewertungen
- Above-Knee Prosthetics: The Knud Jansen LectureDokument15 SeitenAbove-Knee Prosthetics: The Knud Jansen LecturerkNoch keine Bewertungen
- LGN365 Fatloss Routine #2Dokument3 SeitenLGN365 Fatloss Routine #2madmax_mfpNoch keine Bewertungen
- Biomechanics of Hip Joint: A Review: Bhaskar Kumar MadetiDokument19 SeitenBiomechanics of Hip Joint: A Review: Bhaskar Kumar MadetiIrik PalaciosNoch keine Bewertungen
- Base Osteosarcoma 6 May 16Dokument121 SeitenBase Osteosarcoma 6 May 16angelmed_unam2048Noch keine Bewertungen
- 3D Human Body System Model ProposalDokument4 Seiten3D Human Body System Model ProposalAndre Gere AdsuaraNoch keine Bewertungen
- Topic 2-Basics of Folk DancingDokument5 SeitenTopic 2-Basics of Folk DancingAnne Marinelle MontegrandeNoch keine Bewertungen
- Phase 1, Workout 1Dokument2 SeitenPhase 1, Workout 1Valentina SunshineNoch keine Bewertungen
- Henry Vernon Crock M.D., M.S., F.R.C.S., F.R.A.C.S. (Auth.) - Practice of Spinal Surgery-Springer Vienna (1983) PDFDokument334 SeitenHenry Vernon Crock M.D., M.S., F.R.C.S., F.R.A.C.S. (Auth.) - Practice of Spinal Surgery-Springer Vienna (1983) PDFIonut Vlad100% (1)
- KyphosisDokument22 SeitenKyphosisRaiganNoch keine Bewertungen
- Arthroscopy Cutter and Bur Reference GuideDokument1 SeiteArthroscopy Cutter and Bur Reference GuidesinajudheenNoch keine Bewertungen
- HSE302 Exercise ProgrammingDokument1 SeiteHSE302 Exercise ProgrammingAdam MarchantNoch keine Bewertungen
- Sciatica - GrudhrasiDokument27 SeitenSciatica - GrudhrasiGAURAV100% (1)
- Effects of Osteoarthritis and Fatigue On Proprioception of The Knee JointDokument5 SeitenEffects of Osteoarthritis and Fatigue On Proprioception of The Knee JointRosaneLacerdaNoch keine Bewertungen
- Selected Instructional Course LecturesDokument27 SeitenSelected Instructional Course LecturesAhmad ShakirNoch keine Bewertungen
- Crossfit - Strongman ManualDokument37 SeitenCrossfit - Strongman ManualAnonymous 4ggleOQusNoch keine Bewertungen
- Growth and Development of Maxilla Updated (Seminar 1)Dokument42 SeitenGrowth and Development of Maxilla Updated (Seminar 1)Yashica KalyaniNoch keine Bewertungen
- Rga FinalDokument10 SeitenRga Finalapi-355830788Noch keine Bewertungen
- Bone - I BDS Mcq'sDokument6 SeitenBone - I BDS Mcq'sSoumya AnandanNoch keine Bewertungen
- Fractures of Shoulder GirdleDokument268 SeitenFractures of Shoulder Girdlemudassarnati100% (3)