Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Treating Bells PalsyDokument2 SeitenTreating Bells PalsyNur Ilmi SofiahNoch keine Bewertungen
- Response To Antiseizure Medications in Neonates With Symptomatic SeizuresDokument14 SeitenResponse To Antiseizure Medications in Neonates With Symptomatic SeizuresNur Ilmi SofiahNoch keine Bewertungen
- Furosemide Mims EngDokument17 SeitenFurosemide Mims EngNur Ilmi SofiahNoch keine Bewertungen
- Nerve Fibres Detection in Paired Eutopic and Ectopic Endometria From Women With Endometriosis - Correlation With Nerve Growth Factor ExpressionDokument19 SeitenNerve Fibres Detection in Paired Eutopic and Ectopic Endometria From Women With Endometriosis - Correlation With Nerve Growth Factor ExpressionNur Ilmi SofiahNoch keine Bewertungen
- Furosemide Drug ProfileDokument34 SeitenFurosemide Drug ProfileNur Ilmi SofiahNoch keine Bewertungen
- It 5 - Anatomy of The Mental and Neurobehavior Disorders - ErbDokument64 SeitenIt 5 - Anatomy of The Mental and Neurobehavior Disorders - ErbNur Ilmi SofiahNoch keine Bewertungen
- Lama Penggunaan Alat Kontrasepsi Suntik 3 Bulan Dengan Perubahan Berat Badan Pada Akseptor Di Desa Gayaman Kecamatan MojoanyarDokument8 SeitenLama Penggunaan Alat Kontrasepsi Suntik 3 Bulan Dengan Perubahan Berat Badan Pada Akseptor Di Desa Gayaman Kecamatan MojoanyarNur Ilmi SofiahNoch keine Bewertungen
- It Dr. Irsan Shaleh, Antidiabetic Drugs Slide 51Dokument1 SeiteIt Dr. Irsan Shaleh, Antidiabetic Drugs Slide 51Nur Ilmi SofiahNoch keine Bewertungen
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDokument32 SeitenNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdNur Ilmi SofiahNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- POWEV2434234Dokument461 SeitenPOWEV2434234John M. HemsworthNoch keine Bewertungen
- Reported Speech Rd1Dokument3 SeitenReported Speech Rd1Jose ChavezNoch keine Bewertungen
- How To Live A Healthy LifestyleDokument2 SeitenHow To Live A Healthy LifestyleJocelynNoch keine Bewertungen
- Cranial Deformity in The Pueblo AreaDokument3 SeitenCranial Deformity in The Pueblo AreaSlavica JovanovicNoch keine Bewertungen
- Culture and Creative Industries in TanzaniaDokument70 SeitenCulture and Creative Industries in TanzaniaYana ArsyadiNoch keine Bewertungen
- Cri 192Dokument5 SeitenCri 192Reyn CagmatNoch keine Bewertungen
- Oc ch17Dokument34 SeitenOc ch17xavier8491Noch keine Bewertungen
- Hosea - A New Translation With Introduction and Commentary (Anchor Bible 24)Dokument727 SeitenHosea - A New Translation With Introduction and Commentary (Anchor Bible 24)Azoth ImóveisNoch keine Bewertungen
- TTG Basic Rules EngDokument1 SeiteTTG Basic Rules Engdewagoc871Noch keine Bewertungen
- Beed 3a-Group 2 ResearchDokument65 SeitenBeed 3a-Group 2 ResearchRose GilaNoch keine Bewertungen
- Elitmus PapersDokument21 SeitenElitmus Papersanon_879320987Noch keine Bewertungen
- ResumeDokument2 SeitenResumeKeannosuke SabusapNoch keine Bewertungen
- CIR v. San Roque Power Corp., G.R. No. 187485, February 12, 2013Dokument8 SeitenCIR v. San Roque Power Corp., G.R. No. 187485, February 12, 2013samaral bentesinkoNoch keine Bewertungen
- Task 12 - Pages 131-132 and Task 13 - Pages 147-148 (Bsma 2c - Zion R. Desamero)Dokument2 SeitenTask 12 - Pages 131-132 and Task 13 - Pages 147-148 (Bsma 2c - Zion R. Desamero)Zion EliNoch keine Bewertungen
- Cinderella: From The Blue Fairy Book of Andrew LangDokument7 SeitenCinderella: From The Blue Fairy Book of Andrew LangnizamianNoch keine Bewertungen
- Madali V PeopleDokument2 SeitenMadali V PeopleNico NuñezNoch keine Bewertungen
- Adeyinka Wulemat Olarinmoye - The Images of Women in Yoruban Folktales PDFDokument12 SeitenAdeyinka Wulemat Olarinmoye - The Images of Women in Yoruban Folktales PDFAngel SánchezNoch keine Bewertungen
- Grade 3 MathematicsDokument3 SeitenGrade 3 Mathematicsailaine grace alapNoch keine Bewertungen
- Ruchika Project ReportDokument28 SeitenRuchika Project Reportnavdeep2309Noch keine Bewertungen
- IndexDokument3 SeitenIndexBrunaJ.MellerNoch keine Bewertungen
- Sponsorship Details - IIT DelhiDokument4 SeitenSponsorship Details - IIT DelhiRohit KumarNoch keine Bewertungen
- VoorbeeldDokument99 SeitenVoorbeeldRobin VosNoch keine Bewertungen
- Why We're Still Learning New Things About The JFK AssassinationDokument8 SeitenWhy We're Still Learning New Things About The JFK AssassinationNolan SNoch keine Bewertungen
- Victorian AOD Intake Tool Turning Point AuditDokument8 SeitenVictorian AOD Intake Tool Turning Point AuditHarjotBrarNoch keine Bewertungen
- Reading Activity - A Lost DogDokument3 SeitenReading Activity - A Lost DogGigsFloripaNoch keine Bewertungen
- Thompson VarelaDokument18 SeitenThompson VarelaGiannis NinosNoch keine Bewertungen
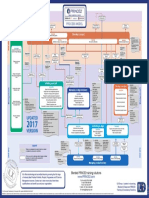
- p2 Process Model 2017Dokument1 Seitep2 Process Model 2017Miguel Fernandes0% (1)
- Spotify Strategig Possining and Product Life Cycle Four Basic Stages.Dokument5 SeitenSpotify Strategig Possining and Product Life Cycle Four Basic Stages.Jorge YeshayahuNoch keine Bewertungen
- Extreme Risk FinanceDokument322 SeitenExtreme Risk FinanceThomas Thomas100% (2)
- Kosem SultanDokument2 SeitenKosem SultanAmaliaNoch keine Bewertungen