Das könnte Ihnen auch gefallen
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionVon EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNoch keine Bewertungen
- Acute Abdomen: - DefinitionDokument27 SeitenAcute Abdomen: - DefinitionWorku KifleNoch keine Bewertungen
- Cme (Tdhi)Dokument64 SeitenCme (Tdhi)OB-Gyne TDHINoch keine Bewertungen
- Oncology Nursing IntensiveDokument75 SeitenOncology Nursing IntensiveVinsuiCzar BaylonNoch keine Bewertungen
- Measles-Outbreak-in-the-Philippines-IH211 (1) - Converted - Compressed PDFDokument11 SeitenMeasles-Outbreak-in-the-Philippines-IH211 (1) - Converted - Compressed PDFlester abadNoch keine Bewertungen
- Therapy - Siti Setiati Evidence Based MedicineDokument33 SeitenTherapy - Siti Setiati Evidence Based MedicinejoeNoch keine Bewertungen
- Gastrointestinal System: Miranda KhidesheliDokument155 SeitenGastrointestinal System: Miranda KhidesheliTanmay NainNoch keine Bewertungen
- Postpartum CollapseDokument54 SeitenPostpartum Collapsemedical chroniclesNoch keine Bewertungen
- Sudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015Dokument23 SeitenSudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015DrChauhanNoch keine Bewertungen
- Abdominal Wall IncisionDokument42 SeitenAbdominal Wall IncisionURo KkuNoch keine Bewertungen
- Lupus Case PresentationDokument48 SeitenLupus Case PresentationRoscelie KhoNoch keine Bewertungen
- Critical Appraisal EBM-Therapy Journal IDokument29 SeitenCritical Appraisal EBM-Therapy Journal IJosephine IrenaNoch keine Bewertungen
- MAM Manual of OperationsDokument144 SeitenMAM Manual of OperationsJames Abram GuardiarioNoch keine Bewertungen
- Doh Programs ShortcutDokument26 SeitenDoh Programs ShortcutSai BondadNoch keine Bewertungen
- Mothers Class Buntis Congress 1Dokument12 SeitenMothers Class Buntis Congress 1Hersy Marie Azores GarayNoch keine Bewertungen
- Abdominal X-RayDokument82 SeitenAbdominal X-RayAzmiyah Febri Pramawardani100% (1)
- Journal Appraisal On Therapeutics - PROBIOTICSDokument43 SeitenJournal Appraisal On Therapeutics - PROBIOTICSLouije MombzNoch keine Bewertungen
- Evidence Based Medicine - CONSORT & AppraisalDokument52 SeitenEvidence Based Medicine - CONSORT & AppraisalNurul Aulia AbdullahNoch keine Bewertungen
- Pediatrics 2 LaboratoryDokument40 SeitenPediatrics 2 LaboratoryAmaetenNoch keine Bewertungen
- Oral Cases Study Guide - PediatricsDokument68 SeitenOral Cases Study Guide - PediatricsJohn100% (1)
- OCHA PH - Measles OutbreakDokument1 SeiteOCHA PH - Measles OutbreakPhilippe Ceasar C. BascoNoch keine Bewertungen
- 01 History Taking and Physical Examination MergedDokument144 Seiten01 History Taking and Physical Examination MergedMohammad Sharid S. SchuckNoch keine Bewertungen
- Basic Wound Closure Knot Tying Primer3Dokument26 SeitenBasic Wound Closure Knot Tying Primer3Louis FortunatoNoch keine Bewertungen
- Gynecology and ObstetricsDokument190 SeitenGynecology and Obstetricsbhesh_seanNoch keine Bewertungen
- IVMS Cell Biology and Pathology Flash Facts IDokument4.999 SeitenIVMS Cell Biology and Pathology Flash Facts IMarc Imhotep Cray, M.D.0% (2)
- Tetanus PDFDokument10 SeitenTetanus PDFVina MuspitaNoch keine Bewertungen
- Pre-Res Case Presentation: Jo Anne N. Ramos, MDDokument72 SeitenPre-Res Case Presentation: Jo Anne N. Ramos, MDKah Mote KyuNoch keine Bewertungen
- How To Read An Abdominal XrayDokument38 SeitenHow To Read An Abdominal Xraytwentyjazzfunkgreats3055100% (1)
- Delirium 1Dokument91 SeitenDelirium 1Jasveen KaurNoch keine Bewertungen
- Systemic Response To Injury IDokument43 SeitenSystemic Response To Injury IPaul BudionganNoch keine Bewertungen
- Course in The WardDokument3 SeitenCourse in The WardAljon S. TemploNoch keine Bewertungen
- CC C C: June 8, 2011 By: Santos, Edilberto DBDokument63 SeitenCC C C: June 8, 2011 By: Santos, Edilberto DBHakugeiNoch keine Bewertungen
- Inserting An NG TubeDokument67 SeitenInserting An NG TubeBalan Andrei MihaiNoch keine Bewertungen
- Gestational Trophoblastic Disease Pt2Dokument75 SeitenGestational Trophoblastic Disease Pt2Abdullah KesalNoch keine Bewertungen
- Community MedicineDokument248 SeitenCommunity MedicineFaisal MahbubNoch keine Bewertungen
- Pediatrics Department Case Presentation Irah Franz D. Flores Block I Group DDokument56 SeitenPediatrics Department Case Presentation Irah Franz D. Flores Block I Group DIrah FloresNoch keine Bewertungen
- E1 Introduction To Community Medicine and Principles of EpidemiologyDokument39 SeitenE1 Introduction To Community Medicine and Principles of EpidemiologyTristen TanNoch keine Bewertungen
- Fatty Liver Disease Ppt-000Dokument55 SeitenFatty Liver Disease Ppt-000Khalid GulNoch keine Bewertungen
- Orientation 2172016Dokument62 SeitenOrientation 2172016Devi Ramadani100% (1)
- Small Group DiscussionDokument3 SeitenSmall Group DiscussionBea SamonteNoch keine Bewertungen
- Introduction To Tropical Medicine and Infectious DiseasesDokument56 SeitenIntroduction To Tropical Medicine and Infectious DiseasesPepe DimasalangNoch keine Bewertungen
- ILA - Hirschsprungs DiseaseDokument48 SeitenILA - Hirschsprungs DiseaseSoleh Ramly100% (1)
- Fatty Liver: Presented By: Mazen Hiresh Jawad Al FoqaraDokument13 SeitenFatty Liver: Presented By: Mazen Hiresh Jawad Al Foqararaed faisalNoch keine Bewertungen
- Mass in Epigastrium-2Dokument37 SeitenMass in Epigastrium-2brown_chocolate87643100% (1)
- Approach To The Diagnosis of Heart Diseases 2Dokument61 SeitenApproach To The Diagnosis of Heart Diseases 2Patricia VirginiaNoch keine Bewertungen
- Dengue DiagnosisDokument160 SeitenDengue DiagnosisBayu Cahyo OktafianNoch keine Bewertungen
- Systemic Response To InjuryDokument58 SeitenSystemic Response To InjuryJustinNoch keine Bewertungen
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDokument36 SeitenMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreNoch keine Bewertungen
- Obstetric FormDokument4 SeitenObstetric FormKhylamarie VillalunaNoch keine Bewertungen
- Printable - Thesis On Bishop ScoreDokument103 SeitenPrintable - Thesis On Bishop Scoreanuaurv100% (3)
- Presented By: Ayu Aqilah Binti Khazani Nurul Dhiya Binti Hassannuddin Narisa Samaradhantia Supervisor: DR .Dr. Khalid Saleh SPPD-KKV, FinasimDokument34 SeitenPresented By: Ayu Aqilah Binti Khazani Nurul Dhiya Binti Hassannuddin Narisa Samaradhantia Supervisor: DR .Dr. Khalid Saleh SPPD-KKV, Finasimekhysyifka0% (1)
- Family Case Report: Quirino Memorial Medical CenterDokument111 SeitenFamily Case Report: Quirino Memorial Medical CenterJanna Janoras ŰNoch keine Bewertungen
- Acute Abdomen in Pregnancy 2Dokument54 SeitenAcute Abdomen in Pregnancy 2jhobarryNoch keine Bewertungen
- Glomerulonephritis PresentationDokument23 SeitenGlomerulonephritis Presentationjacksonyu1234Noch keine Bewertungen
- 2015 Oncology CREOG Review PDFDokument76 Seiten2015 Oncology CREOG Review PDFRima HajjarNoch keine Bewertungen
- Ob-Gyn Review Part 3Dokument101 SeitenOb-Gyn Review Part 3filchibuffNoch keine Bewertungen
- Acute Hypertension-Hypertensive Urgency and Hypertensive EmergencyDokument13 SeitenAcute Hypertension-Hypertensive Urgency and Hypertensive EmergencyAmitKumarNoch keine Bewertungen
- Ob Gyn Sample HisotryDokument4 SeitenOb Gyn Sample HisotrySophia RubiaNoch keine Bewertungen
- Evaluation of Abdominal PainDokument7 SeitenEvaluation of Abdominal PainCherry Faith Merisco LabtangNoch keine Bewertungen
- Study+guide++community+medicine+2010 2011 PDFDokument55 SeitenStudy+guide++community+medicine+2010 2011 PDFArvinth Guna SegaranNoch keine Bewertungen
- Im CPCDokument52 SeitenIm CPCDeepak GhimireNoch keine Bewertungen
- Dengue Deepak 2016 Version OneDokument57 SeitenDengue Deepak 2016 Version OneDeepak GhimireNoch keine Bewertungen
- Diagnosis, Treatment, and Prevention of Typhoid Fever (WHO)Dokument48 SeitenDiagnosis, Treatment, and Prevention of Typhoid Fever (WHO)Nina KharimaNoch keine Bewertungen
- Arteries and Vein of Head and NeckDokument24 SeitenArteries and Vein of Head and NeckDeepak GhimireNoch keine Bewertungen
- Gout CPG Manuscript - PJIM 072808Dokument16 SeitenGout CPG Manuscript - PJIM 072808Francis CastellNoch keine Bewertungen
- Arteries and Vein of Head and Neck PDFDokument24 SeitenArteries and Vein of Head and Neck PDFDeepak GhimireNoch keine Bewertungen
- ToxicityDokument2 SeitenToxicityDeepak GhimireNoch keine Bewertungen
- DTDokument1 SeiteDTDeepak GhimireNoch keine Bewertungen
- Echocardiography DeepakDokument71 SeitenEchocardiography DeepakDeepak Ghimire88% (8)
- Smoking CessationDokument1 SeiteSmoking CessationDeepak GhimireNoch keine Bewertungen
- Viral Exanthems: Study Online atDokument2 SeitenViral Exanthems: Study Online atDeepak GhimireNoch keine Bewertungen
- Sexual Response LectureDokument18 SeitenSexual Response LectureDeepak GhimireNoch keine Bewertungen
- Types of ReflexDokument1 SeiteTypes of ReflexDeepak GhimireNoch keine Bewertungen
- ToxicityDokument2 SeitenToxicityDeepak GhimireNoch keine Bewertungen
- Endocrine SystemDokument41 SeitenEndocrine SystemDeepak Ghimire0% (1)
- Seventh ShiftingDokument1 SeiteSeventh ShiftingDeepak GhimireNoch keine Bewertungen
- Hernia Treatment GeneralDokument2 SeitenHernia Treatment GeneralDeepak GhimireNoch keine Bewertungen
- Introduction To Cosmetic SurgeryDokument2 SeitenIntroduction To Cosmetic SurgeryDeepak GhimireNoch keine Bewertungen
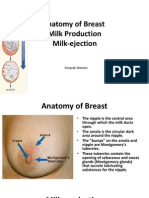
- Anatomy of Breast, Milk Production, and Milk-EjectionDokument23 SeitenAnatomy of Breast, Milk Production, and Milk-EjectionDeepak Ghimire100% (2)
- Wisdom Eye of BuddhaDokument1 SeiteWisdom Eye of BuddhaDeepak GhimireNoch keine Bewertungen
- ReconstructionDokument75 SeitenReconstructionDeepak GhimireNoch keine Bewertungen
- Passport Application FormDokument1 SeitePassport Application FormAl HasaNoch keine Bewertungen
- Endocrine SystemDokument41 SeitenEndocrine SystemDeepak Ghimire0% (1)
- NepalDokument1 SeiteNepalDeepak GhimireNoch keine Bewertungen
- Sleeping Disorders (Somnipathy)Dokument13 SeitenSleeping Disorders (Somnipathy)Deepak GhimireNoch keine Bewertungen
- Student Council 2014/15: ExclusiveDokument3 SeitenStudent Council 2014/15: ExclusiveDeepak GhimireNoch keine Bewertungen
- Clinical Anatomy of Abdominal RegionDokument11 SeitenClinical Anatomy of Abdominal RegionDeepak GhimireNoch keine Bewertungen
- ParasitologiiDokument40 SeitenParasitologiiRabecca TobingNoch keine Bewertungen
- Approach Neurologic DiagnosisDokument8 SeitenApproach Neurologic DiagnosisDeepak GhimireNoch keine Bewertungen
- Succeeding in MRCOG Part IIDokument201 SeitenSucceeding in MRCOG Part IIdrsanamustafa100% (4)
- TCM Menstrual DisordersDokument8 SeitenTCM Menstrual Disorderspranaji100% (7)
- Analisis Determinan Kejadian Berat Bayi Lahir Rendah (BBLR) Di RSUD Tani Dan NelayanDokument7 SeitenAnalisis Determinan Kejadian Berat Bayi Lahir Rendah (BBLR) Di RSUD Tani Dan NelayanchaeworldNoch keine Bewertungen
- Dr. Muh. Ardi MunirDokument6 SeitenDr. Muh. Ardi MunirRahmanNoch keine Bewertungen
- Neonatal Jaundice ThresholdsDokument9 SeitenNeonatal Jaundice ThresholdsMariemma TipianiNoch keine Bewertungen
- Semi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniDokument7 SeitenSemi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniUmar FarooqNoch keine Bewertungen
- Healthcare Cost Containment 1Dokument3 SeitenHealthcare Cost Containment 1Cipta BangunNoch keine Bewertungen
- Alloimmunization in Pregnancy: Brooke Grizzell, M.DDokument40 SeitenAlloimmunization in Pregnancy: Brooke Grizzell, M.DhectorNoch keine Bewertungen
- StainsDokument4 SeitenStainsManikanta Chaitanya LokanadhamNoch keine Bewertungen
- Abo GradingDokument11 SeitenAbo GradingSonu RajuNoch keine Bewertungen
- Twin Stage Part1-HoboDokument13 SeitenTwin Stage Part1-HoboReuben Rajkumar67% (3)
- Presentasi Jurnal LaryngoceleDokument13 SeitenPresentasi Jurnal LaryngoceleTiara Rachmaputeri AriantoNoch keine Bewertungen
- Twin Pregnancy - Labor and DeliveryDokument19 SeitenTwin Pregnancy - Labor and Deliveryrugasa291100% (2)
- General SurgeryDokument83 SeitenGeneral SurgeryCarlos HernándezNoch keine Bewertungen
- Precision AttachmentsDokument92 SeitenPrecision AttachmentsRohan Grover100% (3)
- Tuberculum Sellae MeningiomaDokument9 SeitenTuberculum Sellae MeningiomaFerina Nur HaqiqiNoch keine Bewertungen
- Croatian Society of Radiology (1928-2008)Dokument12 SeitenCroatian Society of Radiology (1928-2008)Anonymous 9QxPDpNoch keine Bewertungen
- Catalogo Medesy 2011Dokument133 SeitenCatalogo Medesy 2011DentaDentNoch keine Bewertungen
- Female Genital CutingDokument80 SeitenFemale Genital CutingTarek AnisNoch keine Bewertungen
- Scars & Devices in Paces 4th Edition PDFDokument132 SeitenScars & Devices in Paces 4th Edition PDFKaleem Ullah Bhatti100% (2)
- Stress and Pregnancy: What Are The Effects?: Can Crying Cause Complications of Pregnancy?Dokument2 SeitenStress and Pregnancy: What Are The Effects?: Can Crying Cause Complications of Pregnancy?Florin TudoseNoch keine Bewertungen
- Nur 460 Capstone Practicum Experience 4Dokument1 SeiteNur 460 Capstone Practicum Experience 4api-449295277Noch keine Bewertungen
- Sonographer Cover LetterDokument8 SeitenSonographer Cover Letterfljyeismd100% (1)
- RSCM - Profil - UkreineDokument13 SeitenRSCM - Profil - UkreineprimastyoanggataNoch keine Bewertungen
- Malposition Malpresentation Abnormal LieDokument41 SeitenMalposition Malpresentation Abnormal Lieapi-3705046100% (1)
- Nogales vs. Capitol Medical CenterDokument34 SeitenNogales vs. Capitol Medical CenterKenneth LimosneroNoch keine Bewertungen
- Diathermy in SurgeryDokument31 SeitenDiathermy in Surgeryrosybash100% (1)
- @. Massive TrasfussionDokument12 Seiten@. Massive TrasfussionYoomiif BedadaNoch keine Bewertungen
- Aseptic Wound Dressing Edited 3 Dec 2008Dokument11 SeitenAseptic Wound Dressing Edited 3 Dec 2008zahisma89Noch keine Bewertungen
- Study On Functional Outcome and Mechanical Failure in Intertrochanteric Femur Fracture Treated With Proximal Femoral Nail antirotation-IIDokument9 SeitenStudy On Functional Outcome and Mechanical Failure in Intertrochanteric Femur Fracture Treated With Proximal Femoral Nail antirotation-IISiddharth JadhavNoch keine Bewertungen