Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Journal of Molecular LiquidsDokument11 SeitenJournal of Molecular LiquidsDennys MacasNoch keine Bewertungen
- Pogon Lifta MRL PDFDokument128 SeitenPogon Lifta MRL PDFMašinsko ProjektovanjeNoch keine Bewertungen
- Lesson Plan For DemoDokument9 SeitenLesson Plan For DemoJulius LabadisosNoch keine Bewertungen
- Music Production EngineeringDokument1 SeiteMusic Production EngineeringSteffano RebolledoNoch keine Bewertungen
- Advanced Herd Health Management, Sanitation and HygieneDokument28 SeitenAdvanced Herd Health Management, Sanitation and Hygienejane entunaNoch keine Bewertungen
- Handbook of Storage Tank Systems: Codes, Regulations, and DesignsDokument4 SeitenHandbook of Storage Tank Systems: Codes, Regulations, and DesignsAndi RachmanNoch keine Bewertungen
- Learning Competency PDFDokument1 SeiteLearning Competency PDFLEOMAR PEUGALNoch keine Bewertungen
- E-CRM Analytics The Role of Data Integra PDFDokument310 SeitenE-CRM Analytics The Role of Data Integra PDFJohn JiménezNoch keine Bewertungen
- Lecture 19 Code Standards and ReviewDokument27 SeitenLecture 19 Code Standards and ReviewAdhil Ashik vNoch keine Bewertungen
- Unit 1 Bearer PlantsDokument2 SeitenUnit 1 Bearer PlantsEmzNoch keine Bewertungen
- BSRM Ultima BrochureDokument2 SeitenBSRM Ultima BrochuresaifuzzamanNoch keine Bewertungen
- Vest3000mkii TurntableDokument16 SeitenVest3000mkii TurntableElkin BabiloniaNoch keine Bewertungen
- Caroline Coady: EducationDokument3 SeitenCaroline Coady: Educationapi-491896852Noch keine Bewertungen
- BAMDokument111 SeitenBAMnageswara_mutyalaNoch keine Bewertungen
- Chapter1 Intro To Basic FinanceDokument28 SeitenChapter1 Intro To Basic FinanceRazel GopezNoch keine Bewertungen
- Fuentes v. Office of The Ombudsman - MindanaoDokument6 SeitenFuentes v. Office of The Ombudsman - MindanaoJ. JimenezNoch keine Bewertungen
- Polyether Polyol Production AssignmentDokument9 SeitenPolyether Polyol Production AssignmentanurdiaNoch keine Bewertungen
- Investment Analysis and Portfolio Management: Frank K. Reilly & Keith C. BrownDokument113 SeitenInvestment Analysis and Portfolio Management: Frank K. Reilly & Keith C. BrownWhy you want to knowNoch keine Bewertungen
- Linux ProgramDokument131 SeitenLinux ProgramsivashaNoch keine Bewertungen
- Bagian AwalDokument17 SeitenBagian AwalCitra Monalisa LaoliNoch keine Bewertungen
- VRARAIDokument12 SeitenVRARAIraquel mallannnaoNoch keine Bewertungen
- Sheetal PatilDokument4 SeitenSheetal PatilsheetalNoch keine Bewertungen
- City Limits Magazine, December 1981 IssueDokument28 SeitenCity Limits Magazine, December 1981 IssueCity Limits (New York)Noch keine Bewertungen
- Abas Drug Study Nicu PDFDokument4 SeitenAbas Drug Study Nicu PDFAlexander Miguel M. AbasNoch keine Bewertungen
- Exclusive GA MCQs For IBPS Clerk MainDokument136 SeitenExclusive GA MCQs For IBPS Clerk MainAnkit MauryaNoch keine Bewertungen
- Post Renaissance Architecture in EuropeDokument10 SeitenPost Renaissance Architecture in Europekali_007Noch keine Bewertungen
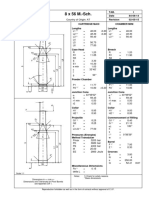
- 8 X 56 M.-SCH.: Country of Origin: ATDokument1 Seite8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNoch keine Bewertungen
- What Is The PCB Shelf Life Extending The Life of PCBsDokument9 SeitenWhat Is The PCB Shelf Life Extending The Life of PCBsjackNoch keine Bewertungen
- WSD M1a283 B50Dokument9 SeitenWSD M1a283 B50'Lampa'Noch keine Bewertungen
- Communication Skill - Time ManagementDokument18 SeitenCommunication Skill - Time ManagementChấn NguyễnNoch keine Bewertungen